Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Jin Hyung Shin
Joong Sook Lee
Ki Hoon Han
Kang Ho Bae
http://dx.doi.org/10.5103/KJSB.2018.28.1.45 Epub 2018 April 13
Abstract
Objective: The purpose of this study was to investigate the effect of foot strengthening exercise program and functional insoles on joint angle and plantar pressure in elderly women. Thirteen elderly women who were enrolled in a university senior citizens academy of a metropolitan city in 2017 were divided into two groups: exercise group with functional insole (n=7) and exercise group without functional insole (n=6).
Method: Three-dimensional motion analysis and Pedar-X were performed to compute the joint angle and the foot plantar pressure, respectively. Two-way repeated measure ANOVA was conducted to compare dependent variables within and between groups. The significance level was set at α =.05.
Results: The range of motion (ROM) of the ankle, knee, and hip joints in the exercise group with functional insole increased significantly more than the exercise group without functional insole. In both the experimental group and the comparison group, the maximum foot plantar pressure and the mean foot plantar pressure were decreased, but the comparison group without functional insole showed more decrease. Since the experimental group demonstrated greater pressure than the comparison group in the contact area (forefoot, midfoot), it was distributed over a greater area.
Conclusion: The results of this study suggest that participation in foot strengthening exercises and using a functional insole has more positive effects than foot strengthening exercises alone on the joint angle and plantar pressure in elderly women. Increased foot plantar pressure led to an increased contact area (forefoot, midfoot) for distribution of the foot plantar pressure, but the effect of reducing the maximum and average plantar pressures was incomplete. However, wearing functional insoles along with exercise, could help in improving the stability of the joints, by increasing the range of motion, and could help the elderly in movement of the muscles more effectively, leading to an improvement in gait function.
Keywords
Foot strengthening exercise Functional insole Range of motion Foot plantar pressure Elderly women
When our ancestors started walking upright on two legs, the feet became an important part for supporting body weight and sustaining body balance. The foot has a complex structure containing 26 bones, 32 muscles and tendons, and 107 ligaments that build an intertwined network. At each step, a load 1.5 times the body weight is applied to the weight-bearing foot, and about 5,000 to 8,000 steps are taken each day (Park, 2017). Despite their important role in sustaining the whole body, we admittedly pay less attention to the feet compared to the rest of our body. Any problems with the foot affect the gait and increase burden on the ankle, knee, and hip joints, as well as the spine, resulting in abnormal body balance. In particular, pes planus (also known as flatfoot or flat foot, pronated feet, or fallen arches), is prevalent both among the elderly and young people. It refers to a condition of sole deformity in which the medial arch of the foot collapses and flattens out, accompanied by rearfoot valgus and forefoot abduction (Sung, 2017). According to the 2015 data released by the Health Insurance Review & Assessment Service in South Korea (cited in Park, 2015), the prevalence of diagnosed flatfoot increased by 25.1% in three years from 15,172 in 2013 to 18,982 in 2015, with young children (< 10 years) forming the highest proportion in 2015 (42.8%), followed by the age bracket of 10~19 years (33.9%). That is, children and youth (< 20 years) accounted for 76.7% of the population diagnosed with flatfoot.
Continuous physical activity in a patient with flat foot leads to excessive unwanted movements in the lower body, which in turn leads to overpronation of the subtalar joint, which is located just below the ankle joint, and causes the medial tibia to undergo rapid rotation, putting the patient at a higher risk of knee injury, compared with the unaffected population (Han, 2014). By inducing changes in the pressure distribution transferred to the weight-bearing foot, depending on the type and direction of loading, flatfoot affects muscle activity and postural alignment, compromising gait and balance and causing muscle pain including back pain (Lee, Chang, & Lee, 2009; Hong, Li, & Fong, 2008). An overpronated foot causes severe pain in the sole, plantar fascia, posterior tibial muscle, anterior tibial muscle, and gastrocnemius muscle, as well as pain, tingling, and numbness in the vestibular nerves, causing frequent pain during walking or exercise (Sharmann, 2010). Therefore, individuals with flat feet have higher energy requirements and feel fatigue in the foot more easily compared to those with normal feet.
The treatment options for flatfoot are largely divided into surgical and conservative methods. The former includes taping, foot orthoses or orthopedic footwear, and foot strengthening exercises. In recent years, there has been a growing interest in the methods applying constant pressure, such as taping, foot orthoses, and foot insoles (Jun, 2015). Supportive or assistive devices such as taping are commonly used to protect the ankle joint from damage and to distribute the foot plantar pressure by sustaining the medial arch higher (Kang, 2008). According to published studies investigating the function of such insoles in conjunction with their shape and material properties, insoles are made of soft materials to prevent injuries likely to occur while walking and their major function is to prevent the feet and lower extremities from being directly affected by excessive external shock (Lim & Lee, 2002). It has also been reported that insoles contribute to distributing foot plantar pressure or decreasing the pressure on a specific area while walking or working in a standing position for long stretches. In particular, customized insoles can mitigate pressure-induced impact and pain by spreading the pressure on a specific area evenly across the entire foot area while walking (Jung et al., 2010). It was also found that an insole with a built-in arch reduced stress on the arch of the foot, with the arch form being maintained longer, as compared to without insoles (Lee & Oh, 2005; Chiu & Wang, 2007; Lott, Hastings, Commean, Smith, & Mueller, 2007; Kogler, Solomonidis, & Paul, 1995).
An earlier study reported that taping, a conservative treatment approach, had the effect of raising the arch, but the positive effect was diminished 48 hours after application (Yoho, 2012). Brown (1995) reported that wearing foot orthotics and specifically designed footwear, which is a passive method of correcting the inappropriate alignment in the flatfoot, can cause atrophy of the foot intrinsic muscles and have a negative long-term effect due to increased reliance on assistive devices. However, studies on other conservative treatment options report that foot strengthening exercises reduce the excessive pronation of the foot and contribute to foot realignment (Jung et al., 2011; Lynn, Padilla, & Tsang, 2012) and that it is a simple method for improving foot function (Panichawit, Bovonsunthonchai, Vachalathiti, & Limpasutirachata, 2015). Murley, Menz, and Landorf (2009) noted that foot shape is closely associated with the function of lower extremity musculature and emphasized the importance of exercise intervention. It was also reported that exercises for strengthening the intrinsic muscles of the foot, such as towel-curl with the toes, short-foot exercise, and toe pick-up, raise the medial arch (Won & Lee, 2010; Jung et al., 2011). A study investigating the effects of foot orthotics on flexible flatfoot in adults reported that concomitant foot muscle strengthening exercises increased the efficacy of foot orthotics compared with a treatment option prescribing only foot orthotics (Park, Kim, & Kim, 2012). Nurse and Nigg (2001) found that foot sensory feedback alteration and lower extremity muscle activity affected the lower extremity alignment. In a study in which foot muscle strengthening exercise program was administered to subjects with flat feet, exercises were found to induce flat foot arch formation, leading to overall benefits such as positive changes in the lower extremity alignment and the lumbar part through (An, 2013).
A large number of studies have been performed on the diagnosis and evaluation, as well as the effects of various conservative treatment options on people with foot deformities including flat feet; however, the biomechanical effects of such conservative treatments have not yet been clearly determined (Kim, 2013). Studies presented so far are mainly concerned with functional evaluation, lacking in objectivity and quantitative analysis, and the findings of those studies have not found sufficient applications in clinical settings. Few studies have investigated the combined effects of functional insoles and foot strengthening exercises in patients with flatfoot. Furthermore, although many studies have investigated gait characteristics associated with insoles, a more in-depth study is required, considering of the numerous variables involved in the effects of functional insoles and foot strength exercises. Most of the previous studies have examined the effects of insoles with respect to foot plantar pressure distribution, and there is a lack of comprehensive studies on joint angles of the lower extremities based on biomechanical movement analysis during walking. Kelly, Cresswell, Racinais, Whiteley, and Lichtwark (2014) noted that plantar intrinsic muscles are important for the arch, under the load exerted on the foot while walking. Earlier studies have reported that foot muscle strengthening exercises are necessary for maintaining foot function and promotion, and more recent studies have proposed that strengthening the foot intrinsic and extrinsic muscles is the most efficient and active intervention for correcting foot pronation that induces arch flattening (Panichawit et al., 2015; Snyder, Earl, O'Connor, & Ebersole, 2009). Based on literature review, it was deemed necessary to establish an efficient intervention involving foot strengthening exercises and functional insoles, and this study was conducted to investigate the effects of such an intervention on joint angles and foot plantar pressure.
1. Participants
Thirteen elderly women found to have degenerative foot deformities were selected as the subjects of this study from among the elderly (≥ 60 years) participating in a university senior exercise program in a district of a metropolitan city. They were randomly assigned to two groups based on BMI: Group A (n=7) with foot strengthening exercises and functional insoles, for eight weeks and Group B (n=6) with foot strengthening exercises only, for eight weeks. The results of statistical analysis of the mean values of the subjects' pretest and posttest measurement results for each test item are summarized below.
Basic physical characteristics of the subjects of this study are outlined in Table 1. No statistically significant intergroup differences were found in age and anthropometric parameters such as height, weight, and BMI.
|
Group |
Age (yrs) |
|
Height (cm) |
|
Weight (kg) |
|
BMI (kg/m2) |
|
M ± SD |
M ± SD |
M ± SD |
M ± SD |
||||
|
A group |
63.71±3.90 |
|
154.31±4.79 |
|
56.84±8.21 |
|
23.91±3.57 |
|
B group |
65.83±4.67 |
|
152.02±4.88 |
|
55.98±4.43 |
|
24.23±1.47 |
2. Measurements
1) Range of motion
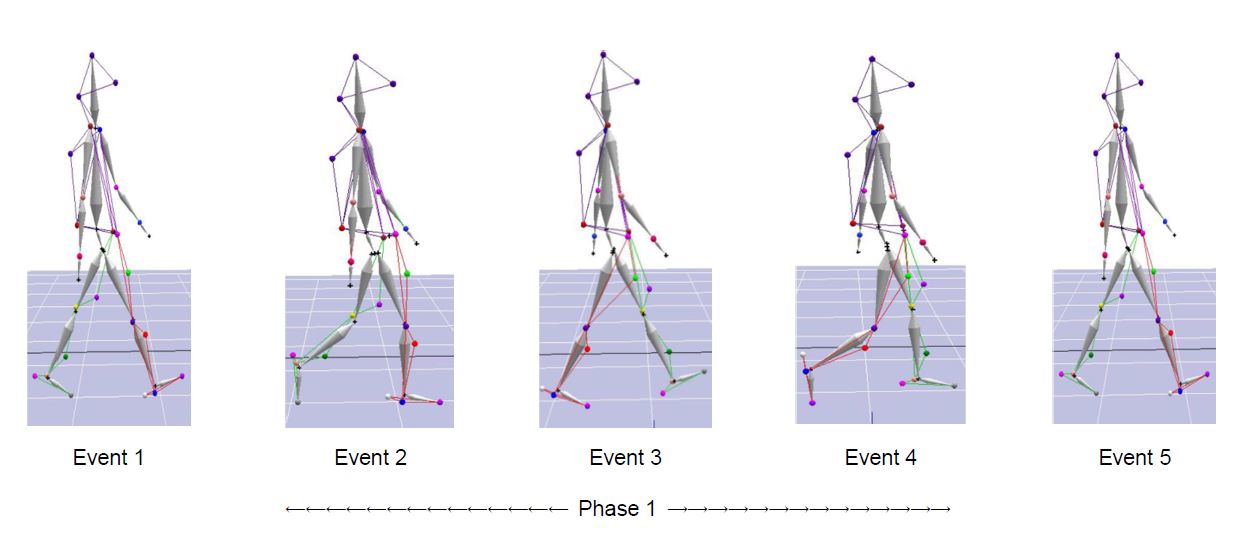
Image data collection during the 10-m walking test was made with five Qualisys infrared cameras that were calibrated prior to measurement using the Nonlinear Transformation (NLT) method. Reflective markers were attached to all segments of the lower extremity joints to enable accurate tracking of in-movement positions from a distance of 10 m while performing 3D motion analysis (Figure 1). In order to minimize data measurement errors, the subjects were instructed to wear the sneakers and workout leggings of the same brand and to walk at a comfortable speed in the motion capture volume, and the mean values were obtained from quintuplicate measurements. The Kwon 3D motion analysis program of VISOL Inc. was used to compare the ranges of motion of ankle plantar flexion-dorsiflexion (x-axis), knee flexion-extension (x-axis), and hip flexion-extension, adduction-abduction, and pronation-supination (x-, y-, and z-axis, respectively). The locations of the reflective markers attached are listed in Table 2 and the analysis interval is illustrated in Figure 1.
|
Measuring item |
Measurement part |
||
|
Front |
Hip joint |
1 Right ASIS 2 Left
ASIS 3 Right GT 4 Left GT 5 Right thigh 6 Left
thigh |
|
|
Knee |
7 Right knee 8 Left knee 9 Right interior knee 10 Left
interior knee |
||
|
Ankle |
11 Right Ankle 12 Left Ankle 13 Right interior ankle 14 Left interior ankle 15 Right toe 16 Left toe |
||
|
Back |
Hip joint |
17 Left PSIS 18 Right PSIS 19 Sacrum |
|
|
Ankle |
20 Left heel 21 Right heel |
||
|
|
|||
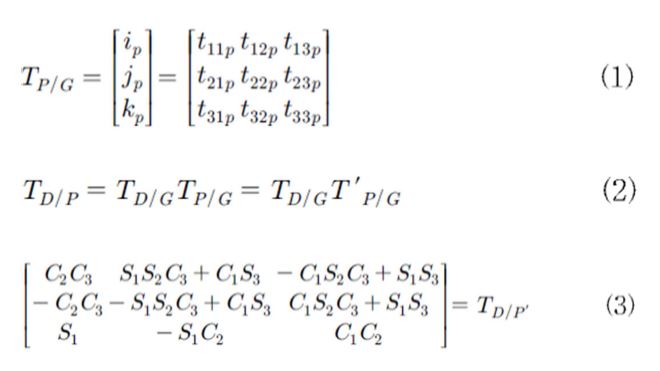
Joint angles were calculated using the equations below (Figure 2), and the joint angles of ankle plantar flexion-dorsiflexion (x-axis), knee flexion-extension (x-axis), and hip flexion-extension, adduction-abduction, and pronation-supination (x-, y-, and z-axis, respectively) were measured and compared using the 3D vector angle calculation formula presented in Kwon (2008), whereby the values excluding the maximum and minimum joint angles were used for ROM analysis). The local reference frame of each segment was defined as per anatomical position (Han et al., 2012). The x-, y-, and z-axis lines were aligned to mediolateral axis, anteroposterior axis, and longitudinal, respectively.
2) Foot plantar pressure
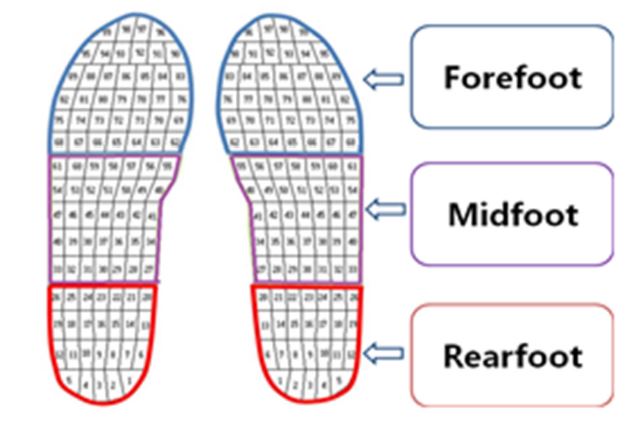
Data for foot plantar pressure was obtained using the Pedar-X system (Novel Gmbh, Germany) that can measure foot pressure distribution through 99 pressure sensors on each side and transmit data directly in the form of Bluetooth signals. For foot plantar pressure measurement, the foot was divided into the forefoot, midfoot, and rearfoot regions (Figure 3), and the pressures exerted on the unit area and each sensor of each section were added up, and the peak and mean foot plantar pressures and contact areas were obtained (Park, Lee, Kim, Yoo, & Kim, 2011). The subjects in Group A were instructed to wear the sneakers of the same brand inserted with insole-type pressure sensors and to walk naturally for 10 meters. Data collection was made by gathering the foot plantar pressure data of the three right-foot steps after excluding the first and last walking data from the quintuplicate measurement.
3. Exercise program
The composition of the exercise program administered in this study for the purpose of assessing the effects of foot strengthening exercises was based on the exercise intervention presented by Prentice (2006). Squats, toe exercises, ankle exercises, walking exercises, and elastic band (Theraband, GmbH, Hadamar, Germany) exercises were administered, with progressively increasing intensity. The intensity of each exercise was assessed by individual perception using the Rate of Perceived Exertion (RPE), based on the Borg's scale. The intensity was set to increase progressively in three steps of RPE 10~11 (weeks 1~3), 12~13 (weeks 4~6), and 14~15 (weeks 7~8). The perceived exertion scale measures the exercise intensity in 6~20 levels. Figure 4 illustrates the Borg (1892) Rating of Exertion Scale.

The exercise program was administered twice a week (60 min per session), and each subject was encouraged to do her best while participating in the exercise program. Table 3 presents the detailed content of the foot strengthening exercises.
|
Exercise type |
Program contents |
Intensity |
Frequency |
|
|
Warm-up (10 min) |
Stretch & Line dance |
- |
1~8 week 2 times/week |
|
|
Main exercise (40 min) |
Foot strength |
Quarter
squat, Half squat, Full squat, Toe extension, Toe curl, Arch exercise, Elastic-band
exercise, Ankle curl, Ankle extension, short foot exercise |
10~20 times (3~5 sets) RPE 11~13 |
|
|
Cool-down (10 min) |
Static stretching |
- |
||
4. Functional insole
The functional insole used in this study is the "arch hard" insole (hardness: 45, C type, peel strength: 63 N/5 cm, arch flattening: maintained at 94%), which was developed based on a mechanism designed to prevent arch deformation, manufactured by Company F in South Korea that participated in the joint research with Woo et al. (2015) and Bae et al. (2016). The "arch hard" insole is easy to use because its arch height can be adjusted and the arch support has a hardness adequate for flatfoot. In particular, the hard wedge forming the arch support has the effect of reducing foot fatigue by spreading the body weight exerted on the foot, mitigating shock, and preventing and correcting flatfoot by stabilizing the calcaneus, as it is designed to comfortably cover the heel. For the purpose of this study, Group A subjects were instructed to replace their insoles with these functional insoles at least one hour per day for eight weeks. Figure 5 is a snapshot of a pair of "arch hard" insoles used in this study.

5. Data processing & Statistical analysis
Data analysis was performed using the SPSS Ver. 23.0 statistical program, with which the means and standard deviations of the general characteristics of the subjects and the variables were obtained. Independent t-test was performed to test the intergroup homogeneity at the pre-measurement stage, and two-way repeated measure ANOVA was performed to compare the effects of the intervention methods between the two groups. The analysis results were considered to be statistically significant at the significance level of α = .05.
1. Range of motion
Table 4 outlines the results of the ROM measurements in both groups in time series. Statistically significant time-dependent and intergroup differences were observed in the left ankle plantar flexion-dorsiflexion, between the time series and groups (F = 6.040, p = .032*), and in the right hip pronation-supination between time series (F = 5.014, p = .047*). Statistically significant time-dependent and intergroup differences were also observed in the left hip pronation-supination (F = 5.650, p = .037*). Comparison of the pretest-posttest results revealed that Group A showed an increase in ROM in all variables, except for the left knee flexion-extension and right hip pronation-supination (decrease), albeit without statistically significant differences. Contrary to this, Group B showed no change or decrease in any variable.
|
Division |
Pre (M ± SD) |
Post (M ± SD) |
F |
p |
|
|
Right |
A group |
33.29±8.43 |
33.90±5.26 |
Time F=.999 Group F=.587 Time × Group F=2.743 |
Time p=.339 Group p=.460 Time × Group p=.126 |
|
B group |
37.02±2.76 |
34.53±1.25 |
|||
|
Left foot X |
A group |
31.19±7.22 |
33.80±5.54 |
Time F=.003 Group F=1.324 Time × Group F=6.040 |
Time p=.957 Group p=.274 Time × Group p=.032* |
|
B group |
36.98±3.48 |
34.48±4.08 |
|||
|
Right |
A group |
64.87±8.06 |
68.40±3.82 |
Time F=.392 Group F=.191 Time × Group F=.630 |
Time p=.544 Group p=.670 Time × Group p=.444 |
|
B group |
65.02±14.31 |
64.60±5.97 |
|||
|
Left knee X |
A group |
67.70±2.68 |
66.34±6.04 |
Time F=1.111 Group F=.869 Time × Group F=.055 |
Time p=.314 Group p=.371 Time × Group p=.819 |
|
B group |
66.30±5.52 |
64.17±2.90 |
|||
|
Right |
A group |
43.57±11.00 |
48.03±4.20 |
Time F=.750 Group F=.004 Time × Group F=.761 |
Time p=.405 Group p=.952 Time × Group p=.402 |
|
B group |
45.40±15.32 |
45.38±17.51 |
|||
|
Left hip joint X |
A group |
49.33±4.86 |
50.41±5.33 |
Time F=.622 Group F=.049 Time × Group F=2.495 |
Time p=.447 Group p=.829 Time × Group p=.143 |
|
B group |
52.02±5.88 |
48.77±2.95 |
|||
|
Right hip joint Y |
A group |
18.53±3.52 |
17.97±4.01 |
Time F=5.014 Group F=1.329 Time × Group F=2.405 |
Time p=.047* Group p=.273 Time × Group p=.149 |
|
B group |
21.55±1.91 |
18.48±2.21 |
|||
|
Left hip joint Y |
A group |
18.74±3.36 |
19.13±3.06 |
Time F=.045 Group F=.010 Time × Group F=.279 |
Time p=.863 Group p=.921 Time × Group p=.608 |
|
B group |
19.53±3.91 |
18.63±3.34 |
|||
|
Right hip joint Z |
A group |
20.69±5.20 |
21.83±6.04 |
Time F=.760 Group F=.055 Time × Group F=1.555 |
Time p=.402 Group p=.819 Time × Group p=.238 |
|
B group |
25.38±15.34 |
18.93±5.58 |
|||
|
Left hip joint Z |
A group |
18.51±3.80 |
22.10±4.60 |
Time F=.022 Group F=.154 Time × Group F=5.650 |
Time p=.885 Group p=.702 Time × Group p=.037* |
|
B group |
22.80±6.59 |
19.63±4.32 |
|||
2. Foot plantar pressure
Table 5 outlines the results of foot plantar pressure measurements in both groups in time series. Statistically significant time-dependent differences were observed in the forefoot peak plantar pressure (F = 7.814, p = .017*) and the mean forefoot plantar pressure (F = 12.128, p = .005**), while the mean forefoot plantar pressure showed statistically significant time-dependent and intergroup differences (F = 5.492, p = .039*). Statistically significant time-dependent differences were also observed in midfoot contact area (F = 5.950, p = .033*). Statistically significant time-dependent differences (F = 5.569, p = .038*) as well as time-dependent and intergroup differences (F = 5.638, p = .037*) were shown in the contact area of the rearfoot region. Comparison of mean values of the pretest-posttest foot plantar pressure revealed that peak and mean foot plantar pressures were reduced in both groups, with Group B (without functional insoles) trending towards greater decreases. As for the contact area of the forefoot and midfoot regions, Group A (exercise + insoles) yielded higher values than Group B (exercise only).
|
Division |
Pre (M ± SD) |
Post (M ± SD) |
F |
p |
|
|
Peak pressure fore (kPa) |
A group |
299.81±64.29 |
256.05±34.95 |
Time
F=7.814 Group
F=.246 Time
× Group F=1.199 |
Time p=.017* Group
p=.630 Time
× Group
p=.297 |
|
B group |
276.71±34.02 |
257.58±30.65 |
|||
|
Peak pressure mid (kPa) |
A group |
111.31±17.82 |
105.98±19.94 |
Time
F=2.175 Group
F=1.543 Time
× Group F=.001 |
Time p=.168 Group p=.240 Time
× Group p=.982 |
|
B group |
121.83±15.80 |
116.67±10.39 |
|||
|
Peak pressure rear (kPa) |
A group |
148.43±32.00 |
149.68±32.40 |
Time
F=2.185 Group
F=3.463 Time
× Group F=3.009 |
Time p=.167 Group p=.090 Time
× Group p=.111 |
|
B group |
184.50±26.96 |
168.83±15.87 |
|||
|
Mean pressure fore (kPa) |
A group |
92.22±9.36 |
91.12±7.24 |
Time
F=12.128 Group
F=.073 Time
× Group F=5.492 |
Time p=.005** Group p=.792 Time × Group p=.039* |
|
B group |
92.10±11.92 |
87.38±11.37 |
|||
|
Mean pressure mid (kPa) |
A group |
31.18±4.43 |
31.03±4.47 |
Time
F=.742 Group
F=.813 Time
× Group F=.574 |
Time p=.407 Group p=.387 Time
× Group p=.464 |
|
B group |
34.53±4.32 |
32.05±7.09 |
|||
|
Mean pressure rear (kPa) |
A group |
97.40±18.68 |
96.04±19.79 |
Time F=3.576 Group F=1.108 Time
× Group F=2.352 |
Time p=.085 Group p=.315 Time
× Group p=.153 |
|
B group |
113.96±22.86 |
100.84±16.11 |
|||
|
Area fore (cm2) |
A group |
54.74±4.98 |
57.18±2.26 |
Time
F=2.171 Group F=.748 Time
× Group F=2.462 |
Time p=.169 Group p=.406 Time
× Group p=.145 |
|
B group |
54.13±4.06 |
54.05±4.81 |
|||
|
Area mid (cm2) |
A group |
43.65±5.16 |
47.69±3.87 |
Time F=5.950 Group F=1.606 Time
× Group F=.804 |
Time p=.033* Group p=.231 Time
× Group p=.389 |
|
B group |
40.89±5.90 |
42.76±8.17 |
|||
|
Area rear (cm2) |
A group |
38.08±1.43 |
36.47±2.16 |
Time F=5.569 Group F=.467 Time
× Group F=5.638 |
Time p=.038* Group p=.509 Time × Group p=.037* |
|
B group |
36.48±2.66 |
36.48±2.37 |
|||
The ankle is the joint that transmits the impact force to the foot, which is the first contact between the ground and the lower extremities while walking, and thus plays an important role in absorbing the shock exerted on the body (Choi, 2003). Kim (2006) compared the ROM measurements between the states before and after wearing foot orthotics in 16 subjects and reported that wearing foot orthotics increased the ROM of the ankle joint absorbing the shock generated when the heel touches the ground. Yang (2009) conducted a study on 30 women patients, diagnosed with degenerative knee osteoarthritis, and reported that muscle exercises increased the muscle mass of the lower extremities and muscle activity, thus increasing the strength of the ankle when the foot lands on the ground and lifts off while walking, which in turn increased the ankle angle. Lee, Lee, Lee, & Park (2007) reported that wearing foot orthotics contributed to the walking comfort of the subjects with flat feet to a greater degree compared with the controls with normal feet by mitigating the joint angle change. This may explain the result of the present study that the ROM of the ankle increased only in Group A (exercise + insoles).
In previous studies, the knee joint played a very important role in absorbing the shock at the moment of landing (Decker, Torry, Wyland, Sterett, & Richard Steadman, 2003; Zhang, Bates, & Dufek, 2000), and a study investigating gender-dependent gait patterns in 10 men and 10 women subjects reported that the knee joint's shock-absorbing function becomes more important as the walking speed increases because the shock increases with the speed (Kim & Cho, 2013). In the present study, the ROM decreased in Group A only in the left knee flexion-extension, whereas it decreased on both sides in Group B, adversely affecting the shock absorption and ideal walking movements. Yamada and Demura (2008) noted that weakened knee extensors can be the cause of frequent foot fatigue, and Karen & Asa (2001) argued that such a state would impede the movements of the lower extremities including the feet, which would then be exposed to increasing impact force from the ground over time. In this regard, further studies appear necessary to investigate the angular velocity of the knee joint and joint moments.
According to Neumann, Grosz, Kelly, Kiefer, & Martens (2009), abduction moment generated by the abduction of the hip joints has an important effect on the posture stability and dynamic movement function of the femur in the facies frontalis while walking. The result of the present study, that an increase in the ROM of the hip joints was observed in Group A subjects who wore functional insoles in addition to performing foot strengthening exercises allows the assumption that wearing functional insoles contributes to developing ideal walking movements through a more efficient absorption of the impact force from the ground by the lower extremity joints.
In this study, peak plantar pressure is defined as the maximum value of the pressure applied to each insole region during the stance phase (Kim & Choi, 2007). The values of the peak and mean foot plantar pressures and contact area were categorized into forefoot, midfoot, and rearfoot regions. Taken together, the peak plantar pressure decreased in both groups. On that note, previous studies on the foot plantar pressure during walking (Choi, 2012; Lee, Lee, Lee, & Park, 2007; Kim, 2011; Kim, 2013; Kim, Chung, Kim, Jung, & Cho, 2010) stated that arch supports or functional insoles play a role in supporting the medial arch and that the peak plantar pressure decreases in proportion to the increase in the insole angle. It was also reported that foot orthotics such as insoles that support the medial arch efficiently control the medial rotation of the talus, reducing the reverse rotational movements of the shank and thigh, and thus help to maintain balance (Chai, Park, & Kim, 2011). This study evaluated the effects of functional insoles worn by the elderly with degenerative ankle overpronation on decreasing the peak plantar pressure, but yielded a result contradictory to those of previous studies in the rearfoot peak plantar pressure in Group A (foot strength exercise + functional insoles). Considering that decreased peak plantar pressure slightly varies from one study to another, a more in-depth study on the rearfoot region is necessary.
In this study, mean plantar pressure is defined as the mean value of the pressure applied to each insole region during the stance phase. Taken together, the mean plantar pressure decreased in both groups, with Group B (without functional insoles) showing a higher degree of decrease. Previous studies regarding foot muscle strengthening exercises reported that the intrinsic muscles are important to the arch of the foot on which loading is applied for a certain length of time and that foot strengthening exercises are required for sustaining and improving foot function. More recent studies also note that strengthening the foot intrinsic and extrinsic muscles is the most active and efficient method to prevent the joint pronation associated with congenital and degenerative flatfoot (Panichawit, Bovonsunthonchai, Vachalathiti, & Limpasutirachata, 2015; Synder, Earl, O'Connor, & Ebersole, 2009). From the results of this study, it is inferred that the foot strength exercise program administered in this study contributed to joint stability and foot balance during the stance phase of walking by stimulating the inner longitudinal axis, which is the most important muscle in the dynamic body-weight sup- port state, and strengthening the tibialis posterior and peroneus longus muscle.
In this study, the contact area is defined by the percentile of the plantar area contacting the ground during the stance phase applied to each insole region. Taken together, the contact area of Group A (foot strengthening exercises + functional insoles) showed increase in the forefoot and midfoot regions, but not the rearfoot region, and that of Group B (foot strengthening exercises only) showed no change or decrease in the contact area. These results are supported by the results of a study (Lee, 2011; Lee, 2010) according to which the contact area of the foot increased in proportion to the insole angle, when the supination and pronation groups were tested while walking with orthotic insoles. These results can be considered tantamount to the results that peak and mean plantar pressures decrease when high-arch footwear or arch-supporting insoles are worn.
In this study, the effects of foot strengthening exercises and functional insoles on joint angles and plantar pressure were investigated. Recruited into this 8-week intervention study with pretest-posttest design were 13 elderly women (≥ 60 years) enrolled in a university senior academy in a metropolitan city. They were assigned to two groups: Group A with foot strengthening exercises and functional insoles and Group B with foot strengthening exercises only. The results of statistical analysis of the mean values of the subjects' pretest and posttest measurement results for each test item are summarized below.
Firstly, Group A (exercise + soles) showed a higher increases in the range of motion (ROM) of the ankle, knee, and hip joints compared with Group B (exercise only) after the eight-week program, with statistically significant differences in some of the items.
Secondly, the peak and mean plantar pressures were reduced in both A and B groups, with the latter (exercise-only group) trending towards larger decrease, and Group A (exercise + insoles) showed a higher increase in the contact area (forefoot and midfoot) than Group B (exercise only), increasing the effect of pressure distribution.
From the overall results of this study, it can be concluded that greater benefits for the joint angles and foot plantar pressure can be drawn from foot strengthening exercises in tandem with functional insoles than from foot strengthening exercises alone. In terms of foot plantar pressure, the functional insoles increased the contact area (forefoot and midfoot) and distributed the plantar pressure, but resulted in negligible reduction in the peak and mean plantar pressures. However, performing foot strengthening exercises with functional insoles is considered to be more beneficial for the walking ability of the elderly, in terms of stability of joints through increased ROM and more efficient muscle activity. It is considered that functional insoles contribute to the walking ability in the elderly, by promoting more efficient muscular movements.
References
1. An, S. J. (2013). A Study on the Effects of Insoles for Pronation and Muscle Strengthening Exercises on Lumbar Structures and Functions. Unpublished Master's Thesis. Graduate School of Rehabilitation Science of Daegu University.
Crossref
2. Bae, K. H., Shin, J. H., Lee, J. S., Yang, J. O., Lee, B. J. & Park, S. B. (2016). Analyses of Plantar Foot Pressure and Static Balance According to the Type of Insole in the Elderly. Korean Journal of Sport Biomechanics, 26(1), 115-126.
Crossref
Google Scholar
3. Borg, G. (1982). Ratings of perceived exertion and heart rates during short-term cycle exercise and their use in a new cycling strength test. International Journal of Sports Medicine, 3(3), 153-158.
Crossref
Google Scholar
4. Brown, G. P., Donatelli, R., Catlin, P. A. & Wooden, M. J. (1995). The Effect of Two Types of Foot Orthoses on Rearfoot Mechanics. Journal of Orthopaedic & Sports Physical Therapy, 21(5), 258-267.
Crossref
Google Scholar
5. Chai, S. W., Park, K. Y. & Kim, Y. S. (2011). The Effects of functional foot orthotics on the balance according to Foot Shape. Journal of Rehabilitation Welfare Engineering & Assistive Technology, 5(1), 47-52.
Crossref
6. Chiu, M. C. & Wang, M. J. J. (2007). Professional footwear evaluation for clinical nurses. Applied Ergonomics, 38(2), 133-141.
Crossref
Google Scholar
PubMed
7. Choi, J. K. (2012). Evaluation for biomechanical effects of custom-made insole on the gait of pes cavus patients. Unpublished Master's Thesis. Graduate School of Chonbuk National University.
Crossref
8. Choi, K. J. (2003). The Analyses of Biomechanical Differences between General Walking Shoe and mBT Functional Walking Shoe. Unpublished Doctor's Dissertation. Graduate School of Sung Kyun Kwan University.
Crossref
9. Decker, M. J., Torry, M. R., Wyland, D. J., Sterett, W. I. & Richard Steadman, J. (2003). Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clinical Biomechanics, 18(7), 662-669.
Crossref
Google Scholar
10. Han, K. H., Como, S. C., Singhal, K., Lee, S., Kim, J., Kim, J. & Kwon, Y. H. (2012). Analysis of the trunk/shoulder complex motion during the golf drives using a 5-segment trunk/shoulder model. In E. J. Bradshaw, A. Burnett & P. A. Hume (Eds.), Scientific proceedings of the 30th international society of biomechanics in sports conference (pp. 59-62). Melbourne, Australia: Australian Catholic University.
Crossref
Google Scholar
11. Han, S. M. (2014). The effects of arch-formation exercises on the lower leg alignment & physical factors of basketball players with flexible flat foot. Unpublished Doctor's Dissertation. Graduate School of Sejong University.
Crossref
12. Hong, Y., Li, J. X. & Fong, D. T. P. (2008). Effect of prolonged walking with backpack loads on trunk muscle activity and fatigue in children. Journal of Electromyography and Kinesiology, 18(6), 990-996.
Crossref
Google Scholar
13. Jun, Y. T. (2015). The Effect of Pes Planus on Balance and Gait in Kinesio Taping. Unpublished Master's Thesis. Graduate School of Gachon University.
Crossref
14. Jung, D. Y., Kim, M. H., Koh, E. K., Kwon, O. Y., Cynn, H. S. & Lee, W. H. (2011). A comparison in the muscle activity of the abductor hallucis and the medial longitudinal arch angle during toe curl and short foot exercises. Physical Therapy in Sport, 12(1), 30-35.
Crossref
Google Scholar
15. Jung, J. Y., Kim, J. H., Kim, K., Trieu, P. H., Won, Y. K., Kwon, D. K. & Kim, J. J. (2010). Evaluation of Insole-equipped Ankle Foot Orthosis for Effect on Gait based on Biomechanical Analysis. Korean Journal of Sport Biomechanics, 20(4), 469-477.
Crossref
Google Scholar
16. Kang, H. J. (2008). The Effect of a Customized Insole for High-arched Patients with Hindfoot Supination. Unpublished Master's Thesis. Graduate School of Health and Environment Yonsei University.
Crossref
17. Karen, M. & Asa, K. (2001). Standing and very slow walking: foot pain-pressure threshold, subjective pain experience and work activity. Applied Ergonomics, 32, 81-90.
Crossref
Google Scholar
18. Kelly, L. A., Cresswell, A. G., Racinais, S., Whiteley, R. & Lichtwark, G. (2014). Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. Journal of the Royal Society Interface, 11(93), 1-9.
Crossref
Google Scholar
PubMed
19. Kim, D. Y. & Choi, S. B. (2007). Transactions: The Research on Functional Midsole that can Minimize Forefoot Pressure - Focusing on High-Heeled Pumps Type. Journal of the Korean Society of Clothing and Textiles, 31(2), 258-268.
Crossref
Google Scholar
20. Kim, E. H., Chung, J. W., Kim, S. S., Jung, T. W. & Cho, H. K. (2010). The Biomechanical Evaluation of Functional Insoles. Korean Journal of Sport Biomechanics, 20(3), 345-353.
Crossref
Google Scholar
21. Kim, G. (2013). Plantar Pressure and Gait Ability Analysis for Foot Deformities with Arch Support. Unpublished Doctor's Dissertation. Graduate School of Dongshin University.
Crossref
22. Kim, K. H. (2011). Biomechanical Analysis of Arch Support Devices on Normal and Low Arch. Unpublished Master's Thesis. Graduate School of Kyungsung University.
Crossref
23. Kim, R. B. & Cho, J. H. (2013). An Analysis on the Contribution of Lower Limb Joint According to the Gender and Gait Velocity. Korean Journal of Sport Biomechanics, 23(2), 159-167.
Crossref
Google Scholar
24. Kim, S. J. (2006). Correctional Function of Custom Foot Orthotics for Foot Diseases related to Excessive Pronation during Gait. Korean Journal of Sport Biomechanics, 16(1), 65-79.
Crossref
Google Scholar
25. Kogler, G. F., Solomonidis, S. E. & Paul, J. P. (1995). In vitro method for quantifying the effectiveness of the longitudinal arch support mechanism of a foot orthosis. Clinical Biomechanics, 10(5), 245-252.
Crossref
Google Scholar
26. Kwon, Y. H. (2008). Measurement for deriving kinematic parameters: Numerical methods. Handbook of Biomechanics and Human Movement Science, 156-181.
Crossref
Google Scholar
27. Lee, C. M. & Oh, Y. J. (2005). The Development of the Insole for Gait Load Decreasing by Biomechanics Analysis. Journal of the Ergonomics Society of Korea, 24(4), 23-30.
Crossref
Google Scholar
28. Lee, H. T. (2010). The Effect of the Wedge Insole Angle of Supinated Group on Foot Contact Time, Foot Contact Area and Foot Pressure While Walking. Unpublished Master's Thesis. Graduate School of Pukyong National University.
Crossref
Google Scholar
29. Lee, J. H., Lee, Y. S., Lee, J. O. & Park, S. H. (2007). Biomechanical Gait Analysis and Simulation on the Normal, Cavus and Flat Foot with Orthotics. The Korean Society of Mechanical Engineers, 31(11), 1115 -1123.
Crossref
Google Scholar
30. Lee, J. I. (2011). The Effect of Wedge insole of Pronated Group on Maximum Force. Unpublished Master's Thesis. Graduate School of Pukyong National University.
Crossref
31. Lee, S. Y., Chang, J. S. & Lee, M. H. (2009). The Effects of Plantar Foot Pressure and EMG Activation of Neck, Lumbar and Low by Using Carrier during Walking. Korean Journal of Sport Biomechanics, 19(2), 237-244.
Crossref
Google Scholar
32. Lim, G. Y. & Lee, S. D. (2002). The Characteristic Evaluation of Rear Foot Pressure by Impact Shock during Running and Jumping. Journal of the Korean Institute of Plant Engineering, 7(1), 79-87.
Crossref
33. Lott, D. J., Hastings, M. K., Commean, P. K., Smith, K. E. & Mueller, M. J. (2007). Effect of footwear and orthotic devices on stress reduction and soft tissue strain of the neuropathic foot. Clinical Biomechanics, 22(3), 352-359.
Crossref
Google Scholar
34. Lynn, S. K., Padilla, R. A. & Tsang, K. K. (2012). Differences in static- and dynamic-balance task performance after 4 weeks of intrinsic-foot-muscle training: The short-foot exercise versus the towel-curl exercise. Journal of Sport Rehabilitation, 21(4), 327-333.
Crossref
Google Scholar
35. Murley, G. S., Menz, H. B. & Landorf, K. B. (2009). Foot posture influences the electromyographic activity of selected lower limb muscles during gait. Journal of Foot and Ankle Research, 2(35), 1-9.
Crossref
Google Scholar
36. Neumann, D. A., Grosz, C. M., Kelly, E. R., Kiefer, C. & Martens, K. (2009). Kinesiology of the musculoskeletal system: foundations for physical rehabilitation. St. Louis: Mosby.
Crossref
37. Nurse, M. A. & Nigg, B. M. (2001). The effect of changes in foot sensation on plantar pressure and muscle activity. Clinical Biomechanics, 16(9), 719-727.
Crossref
38. Panichawit, C., Bovonsunthonchai, S., Vachalathiti, R. & Limpasutirachata, K. (2015). Effects of Foot Muscles Training on Plantar Pressure Distribution during Gait, Foot Muscle Strength, and Foot Function in Persons with Flexible Flatfoot. Journal of the Medical Association of Thailand, 98(5), 12-17.
Crossref
Google Scholar
39. Park, J. H. (2017, May, 19). Is the foot disease only middle-aged? Spring / Summer 20 Reasons for Diabetic Foot Patient. Bridgenews. Retrieved from http://www.viva100.com/main/view.php?key=2017- 0519020019942.
Crossref
40. Park, J. H., Kim, J. S. & Kim, K. (2012). The Effect of Foot Strengthening Exercise to Young of Hallux Valgus with Flexible Flatfoot. Journal of the Korea Academia-Industrial cooperation Society, 13(11), 5211-5217.
Crossref
Google Scholar
41. Park, S. B., Lee, K. D., Kim, D. W., Yoo, J. H. & Kim, K. H. (2011). Comparative Analysis of Foot Pressure Distribution by Functional Insole to be Transformed and Restored during Walking. Korean Journal of Sport Biomechanics, 21(2), 231-241.
Crossref
Google Scholar
42. Prentice, W. E. (2009). Rehabilitation Techniques in Sports Medicine (4th ed.). New York: Hill Higher Education.
Crossref
43. Sharman, S. A. (2010). Movement system impairment syndrome of the extremities, cervical and thoracic spines. St. Louis, Missouri: Elsevier Mosby.
Crossref
44. Snyder, K. R., Earl, J. E., O'Connor, K. M. & Ebersole, K. T. (2009). Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clinical Biomechanics, 24(1), 26-34.
Crossref
Google Scholar
45. Sung, J. W. (2017). Effects of Korean Medical Treatment Combined with Foot Orthotics on Patients' Center of Gravity with Flat Foot: a retrospective study. Un- published Master's Thesis. Graduate School of Dong-Eui University.
Crossref
46. Won, K. H. & Lee, M. G. (2010). Effects of a strength exercise training for foot intrinsic muscle on height of medial longitudinal arch and balance in females aged 20's. Exercise Science, 19(4), 351-360.
Crossref
47. Woo, J. H., Lee, J. S., Yang, J. O., Lee, B. J., Bae, K. H., Han, D. W., Park, S. M. & Bae, J. W. (2015). Analysis of Plantar Foot Pressure according to Insole Types during Treadmill Gait. Korean Journal of Sport Biomechanics, 25(1), 113-122.
Crossref
Google Scholar
48. Yamada, T. & Demura, S. (2008). Relationships between ground reaction force parameters during a sit-to-stand movement and physical activity and falling risk of the elderly and a comparison of the movement characteristics between the young and the elderly. Archives of Gerontology and Geriatrics, 10, 10-16.
Crossref
Google Scholar
49. Yang, S. M. (2009). Variations in Lower Limb Muscle Activity, Gait Pattern and Pain Variables of Degenerative Gonitis Cases after Aquatic Exercise and Nordic Walking. Unpublished Doctor's Dissertation. Graduate School of Kangnung National University.
Crossref
50. Yoho, R., Rivera, J. J., Renschler, R., Vardaxis, V. G. & Dikis, J. (2012). A biomechanical analysis of the effects of Low-Dye taping on arch deformation during gait. The Foot, 22(4), 283-286.
Crossref
Google Scholar
PubMed
51. Zhang, S. N., Bates, B. T. & Dufek, J. S. (2000). Contributions of lower extremity joints to energy dissipation during landings. Medicine and Science in Sport and Exercise, 32(4), 812-819.
Crossref
Google Scholar
