Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Woo Ram Yoon
Sang Heon Park
Chan Hyeok Jeong
Ji Ho Park
Suk-Hoon Yoon
http://dx.doi.org/10.5103/KJSB.2018.28.1.37 Epub 2018 April 13
Abstract
Objective: The aim of this study was to analyze muscle activation of the lower extremities as a function of changes of the center of pressure (CoP) of the foot during squats in order to provide quantitative information to trainers who would like to teach correct movements for developing muscles.
Method: Ten men with over three years of weight training experience participated in this study (age: 26.1 ± 0.8 yrs, height: 171.2 ± 3.9 cm, body mass: 71.1 ± 5.7 kg, 60%RM: 84 ± 9 kg, career: 4.0 ± 0.7 yrs). The participants were instructed to perform a squat in each of 3 conditions, with different CoP's (the front, middle, and rear of the foot).
Results: The position of the CoP showed significant differences according to instructions in both the eccentric and concentric contraction phases (p < .05). The range of movement of the hip and ankle joints showed significant differences corresponding to changes of the CoP position (p < .05). The rectus femoris and gluteus maximus muscle showed significant differences for different CoP positions only in the concentric contraction phase, while the gastrocnemius and anterior tibialis were significantly different in both the concentric and eccentric contraction phase (p < .05).
Conclusion: When the target muscle of squat training is the gastrocnemius, the CoP should be located in the front of the foot for effective muscle training. When the target muscles of squat training are the gluteus maximus and quadriceps femoris, the CoP should be located on the rear of the foot.
Keywords
Weight training Squat Center of pressure Muscle activation Joint range of motion
The amount of physical activity people engage in has been decreasing, as they spend more time sitting (Oh, Kang, Kwon & Min, 2015). Accordingly, many individuals choose to exercise as a way to improve quality of life through leisure activities, investing great amounts of time and effort (Baik & Shin, 2009; Jung & Chae, 2017; Lee, Lee & Seok, 2008). Weight training is a physical activity to which individuals can have easy access and can do at a relatively low cost, without a great impact on time and the environment. It is widely used by the general public to strengthen the body and promote health, and also by professional athletes to improve their performance (Back, 2016).
In weight training, the calf raise, leg extension, leg curl, leg adduction, leg press, and squat are the main exercises to strengthen the lower extremities, and the squat is the most widely used among them (Chae, Jeong & Jang, 2007; Won, Kim, Bae & Kim, 2013). The squat exercise increases muscle strength and power in the lower extremities, and strengthens lower body muscles and core muscles, including the quadriceps, biceps femoris, gluteus maximus, and gastrocnemius (Escamilla, 2001). In addition, during the squat the entire body is influenced by gravity, as opposed to other types of lower body exercise in which all body parts are fixed except those intended to be strengthened. It is a complex exercise that affects not only ankles, knees, and the hip joint but also the waist. Hence, it is an exercise with multiple advantages. However, it is difficult to maintain a good posture during the squat (Cho, 2005; Fry, Smith & Schilling, 2003; Lander, Bates & Devita, 1986; Won, Kim, Bae & Kim, 2013). To obtain a correct squat posture, it is important to understand functional body movements, which can be explained via interconnected muscle groups, i.e., muscle slings.
A muscle sling is involved in multi-joint movement, distributes load across the joints, and provides the proximal body parts with stability so that distal body parts can be moved accurately. Generally, muscles in a sling are linked with each other by connections at the origin of adjacent muscles, through a structure in which the point contacted by a muscle becomes a pivot point (Page, Frank & Lardner, 2010). The upper and lower bodies are connected in the trunk where the erector spinae and the ipsilateral gluteus maximus pass along the lumbar spine (Gracovetsky, 1997). The lower body is conceptualized as divided into the extensor sling and the flexor sling. The extensor sling consists of the gluteus maximus, quadriceps, and gastrocnemius, and is involved in the extension of the hip and knee and plantar flexion at the ankle; whereas the flexor sling consists of iliopsoas, biceps femoris, and tibialis anterior, each involved in the flexion of the hip, the flexion of the knee, and dorsiflexion at the ankle (Myers, 2001). For example, during the squat the flexor sling is used due to the flexions of the hip and knees and dorsiflexion at the ankles, and simultaneously an eccentric con- traction occurs in the extensor sling. Co-contraction of 2 sling groups provides a functional muscle recruitment pattern corresponding to the multi-joint movement (de Looze, Toussaint, van Dieen & Kemper, 1993). According to a previous study, if the center of pressure (CoP) shifts toward the heel during squat, muscle activation of the tibialis anterior increases and that of biceps femoris also increases, as plantar flexion torque decreases. Conversely, if the CoP shifts toward the toes, muscle activation of the gastrocnemius increases and the quadriceps shows strong activation, as plantar flexion torque and knee extension torque increase (Dionisio, Almeida, Duarte & Hirata, 2008). Thus, even when the same squat movement is performed, the load may not be applied precisely to the target muscle depending on the position of CoP, because muscle activation of the gastrocnemius or the tibialis anterior increases instead of co-contraction. Therefore, it is critical for a squat performer to understand correct squat posture and practice it.
A review of studies on CoP during the squat shows the following. Bak, Shin and Shin (2015) reported in a study on CoP during the squat according to skill level that CoP was more posterior in the experienced group than in the inexperienced group. Da, Lee and Kim (2015) showed that the CoP shifted toward the heel as the squat depth increased, and Lee, Nam and Kim (2013) found that the CoP was located more posteriorly during back squats than during front squats. Kim, Seo, Jung, Lee and Jung (2013) and Kim et al. (2014) reported that doing squats on an unstable surface improved the ability to control CoP. The previous studies on the squat exercise with different CoP's, however, only examined differences in CoP according to the method of squat performance and the posture during squatting, and did not make a meaningful contribution regarding an actual application of the study results. That is, research is lacking on changes occurring in the lower extremity muscles if the CoP on the sole of the foot changes while the same posture is maintained.
Accordingly, this study aimed to examine changes in muscle activation in the lower extremities and changes in posture in relation to changes in the CoP (front, middle, and rear) during squatting, and to provide scientific evidence that can be utilized in practice when trainers or individuals performing the squat to perform the exercise in the way that most effectively develops the target muscles.
1. Participants
The study subjects were 10 men in their 20's who had continuously done weight training for at least 3 years and had no physical injury in the most recent 6 months. They were recruited from a weight training club at K University. The participants' characteristics are shown in (Table 1).
The study was approved by K University Research Ethics Committee. The participants voluntarily agreed to participate in study.
|
Age |
Height |
Body mass |
60%RM |
Career |
|
26.1±0.8 |
171.2±3.9 |
71.1±5.7 |
84±9.0 |
4.0±0.7 |
2. Measurements
The experiment was conducted in the Sports Biomechanics Laboratory at K University. The one-repetition maximum force (1RM) was measured in all participants a week before experiment to establish the baseline load, using the method recommended by the US National Strength & Conditioning Association (NSCA), in the following manner (Beachle & Earle, 2000). Participants warmed up with a weight which they could lift 5~10 times, and then took a one-minute rest. They repeated this 3~5 times, gradually increasing the weight by 15~20 kg and taking a rest for 2 minutes between sets. If they performed a squat movement successfully, the weight was increased, and the measurement was repeated in the same manner. If participants succeeded for one trial after a 2-4-minute rest, the weight was recorded as the 1RM. If they succeeded for more than one trial, the weight was increased by 10~20% after a 2-4-minute rest and the measurement was repeated until they succeeded for only one trial. If they failed, they had a 2-4-minute rest, the weight was reduced by 5~10%, and the measurement was repeated until they succeeded. To minimize the effect of muscle fatigue, all measurements were performed in less than 5 sets.
Before the measurements for the study were taken, participants did the same warm-up exercise they did for the 1RM measurement so that they could perform correct squat movements. To conduct movement analyses, a total of 8 infrared cameras (Oqus 300+, Qualisys, Sweden) were arranged anterior, posterior, and lateral (left and right) to where the participants would perform the squat. To measure the ground reaction force of each leg, 2 ground reaction force plates (Type9286AA, Kistler, Switzerland) were placed as shown in (Figure 1). The rate of sampling was set to 100 Hz for the infrared cameras and 1,000 Hz for the ground reaction force plates.
For segment modeling of the lower extremities, 24 markers made by the researchers were attached to joint points and segment surfaces of the participants. To measure muscle activation, wireless electromyography (zerowire, Aurion, Italy) was used with the rate of sampling set to 1,000 Hz. The infrared cameras, ground reaction force plates, and the equipment to measure muscle activation were connected through an A/D board and tuned using the Qualisys Track Manager program [QTM] (Qualisys, Sweden).
To normalized the electromyogram (EMG) across participants, the maximum voluntary isometric contraction (MVIC) was measured in a squatting posture with the thighs parallel to the ground. The participants were instructed to perform a squat in each of 3 conditions, with different CoP's. The 3 CoP conditions used in the current experiment placed the CoP in the front, middle, and rear of the foot. Participants were provided with detailed explanations before performing the squat in each condition. Specifically, in the condition with the CoP at the front of the foot they were instructed with the terms used by coaches or trainers in the field, and told to "push the ground by moving your force toward the toes." In the conditions with the CoP in the middle and rear of the foot, respectively, they were instructed to "push the ground, maximally balancing between toes and heel" and to "push the ground by moving your force toward the heel." In each of the conditions, participants performed 3 squats with a weight of 60% of the 1RM and rested for 2 minutes between trials.

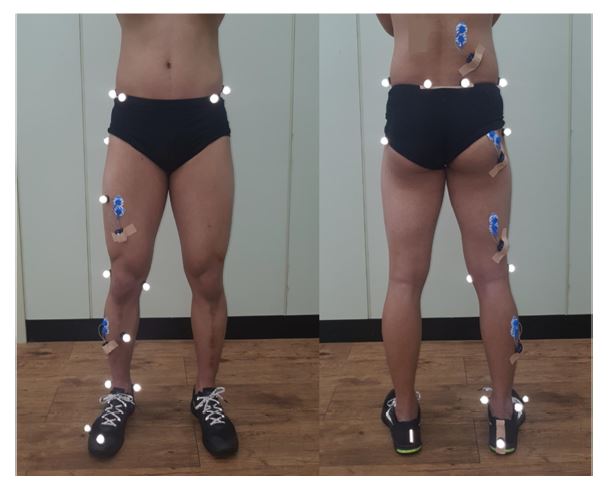
3. Data processing
Data were processed using Matlab2014b (Mathworks, USA). Three-dimensional spatial coordinates were determined from the imaging data obtained by the 8 infrared cameras, using a non-linear transformation (NLT) method. To model the segments in the lower extremities, a total of 17 reflective markers were attached to landmarks in the right lower limbs of the participants (Figure 3). Each of the 2 ground reaction force plates had markers at the 4 corners to determine the coordinates, with Fx indicating the left direction, Fy the front, and Fz the vertical direction (+). To remove error due to noise during measurement, the signals were filtered using a second order Butterworth low-pass filter, with the cutoff frequency set to 6 Hz. Prior to analysis, the EMG data were normalized as percentages with respect to the previously measured MVIC value. To remove noise from the EMG, the data were filtered by a band-pass filter with cutoff frequencies of 20 and 450 Hz, and the filtered data were then quantified into root mean square (RMS) values.
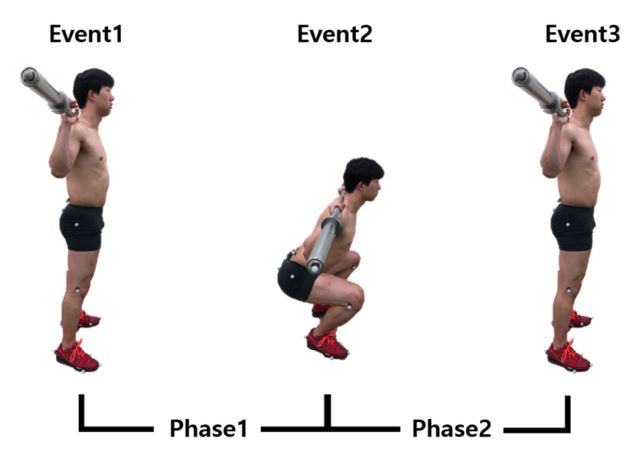
4. Event and phase
To analyze differences in muscle activation and range of motion (ROM) of the lower extremities according to the position of the CoP, the squat process was broken down into 3 events and 2 phases as shown in (Figure 2). Event 1 was defined as the time immediately before the end of the barbell dropped in the vertical direction, Event 2 as the time at which the end of the barbell was positioned at the lowest level, and Event 3 as the time at which the barbell was raised again and its end arrived at its vertical location in Event 1. Phase 1 was defined as the eccentric contraction phase between Events 1 and 2, and Phase 2 as the concentric contraction phase between Events 2 and 3.
5. Analysis of variables
1) Range of motion (ROM)
The joint angles used to compute the range of motion were measured with the use of 3-dimensional positioning coordinates obtained by the infrared cameras. Angles at the joints in the lower extremities (i.e., ankle, knee, and hip) were measured during the squat, and the ROM was computed based on the difference between the angles at maximum extension and maximum flexion at each joint.
2) EMG in the lower extremities
To minimize skin resistance for EMG recording, hair in the areas where EMG electrodes would be attached was shaved and the skin was wiped with alcohol. Electrodes were attached over the erector spinae, gluteus maximus, biceps femoris, rectus femoris, gastrocnemius, and tibialis anterior of the right leg. The sites at which electrodes were attached in the muscles were as follows. For the erector spinae (the longest muscle; longissimus), an electrode was attached laterally at a distance of about 2 finger segments from L1. For the gluteus maximus, an electrode was attached where the hip protruded the most along the greater trochanter of the femur, halfway between the sacrum and lumbar vertebra. For the biceps femoris, an electrode was attached half- way between the ischial tuberosity and the lateral epicondyle of the tibia, and for the rectus femoris, an electrode was attached halfway between the anterior inferior iliac spine and the patella. For the gastrocnemius, an electrode was attached about 1/3 of the way from the head of the fibula to the heel, and for the tibialis anterior, an electrode was attached about 1/3 of the way from the end of the fibula to the medial malleolus (Figure 3). For the sites where electrodes were attached, SANIAM (Surface Electromyography for the Non-Invasive Assessment of Muscles) was referenced (Hermans et al., 1999).
The values of muscle activation during the squat were averaged separately for the eccentric contraction and concentric contraction phases and normalized by dividing by the previously measured MVIC.
: Mean EMG during movement
: Mean maximum voluntary isometric contraction
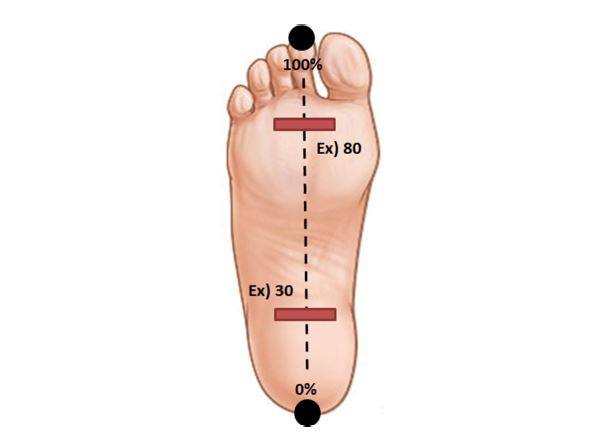
3) Center of Pressure [CoP]
The CoP during the squat was measured in each participant to quantitatively test for changes in CoP in the foot in accordance with the 3 instructions (CoP in the front, middle, and rear of the foot). To confirm the change in plantar CoP during the squat, markers were attached in the lower area of the ground reaction force plates, and 2 additional markers were attached to identify the sole of each participant's foot (as shown in (Figure 4)) to normalize the positions of the CoP for varying foot lengths (heel to toe).
6. Statistical analysis
To examine differences in muscle activation, CoP, and ROM in the lower extremities according to the 3 CoP instructions (the front, middle, and rear of the foot) during the squat, one-way repeated measures ANOVA was performed with Bonferroni correction as a post-hoc test. All data analysis was conducted using SPSS 24.0 (IBM, USA), and the statistical significance level was set to α = 0.05.
The results of the analyses performed on CoP, muscle activation, and ROM were as follows.
To confirm whether the CoP shifted in accordance with the instructions to move it, the CoPs were analyzed. The results showed that in both the eccentric contraction and concentric contraction phases, the CoPs were statistically significantly different across the instructions (Table 2, p < .05).
Regarding difference in ROM in the lower extremities according to the change in CoP, the difference was statistically significant at the hip and the ankle (Table 3, p < .05) but not at the knee (Table 3, p > 0.05).
The estimated muscle activations according to the change in CoP are presented in (Table 4). In the rectus femoris and the gluteus maximus, there was a significant difference in the concentric contraction phase only, whereas in the gastrocnemius and the tibialis anterior the difference was significant in both eccentric contraction and concentric contraction phases (Table 4, p < .05).
|
Variables |
Front (a) |
Middle (b) |
Rear (c) |
F |
p |
Post-hoc |
|
Mean ± SD |
||||||
|
Phase1 CoP |
70.08±19.19 |
65.58±17.13 |
59.80±17.95 |
28.028 |
.000* |
c<b<a |
|
Phase2 CoP |
73.09±19.43 |
68.74±18.77 |
62.95±20.05 |
36.549 |
.000* |
c<b<a |
|
Variables |
Front (a) |
Middle (b) |
Rear (c) |
F |
p |
Post-hoc |
|
Mean ± SD |
||||||
|
Hip ROM |
108.94±9.44 |
107.95±10.80 |
110.92±11.70 |
4.825 |
.021* |
b<c |
|
Knee ROM |
107.23±8.99 |
108.26±8.79 |
108.07±9.41 |
.569 |
.576 |
|
|
Ankle ROM |
31.83±4.13 |
31.51±3.57 |
29.99±5.06 |
5.642 |
.013* |
c<a |
|
Variables |
Front (a) |
Middle (b) |
Rear (c) |
F |
p |
Post-hoc |
|
|
Mean ± SD |
|||||||
|
Erector spinae |
P1 |
2.94±1.11 |
2.25±1.11 |
2.82±1.06 |
1.778 |
.197 |
|
|
P2 |
3.39±1.31 |
3.30±1.34 |
3.40±1.33 |
.888 |
.448 |
||
|
Gluteus maximus |
P1 |
11.17±7.68 |
11.37±7.64 |
12.31±8.79 |
.992 |
.412 |
|
|
P2 |
32.31±14.49 |
30.20±14.05 |
33.12±18.13 |
9.929 |
.007* |
b<c |
|
|
Biceps femoris |
P1 |
2.48±0.93 |
2.32±1.09 |
2.41±0.87 |
.542 |
.575 |
|
|
P2 |
5.54±2.45 |
4.84±1.99 |
5.08±2.20 |
2.914 |
.112 |
||
|
Rectus femoris |
P1 |
1.77±1.35 |
2.03±.98 |
2.28±1.06 |
3.603 |
.077 |
|
|
P2 |
3.21±3.35 |
4.04±3.92 |
4.25±3.87 |
10.288 |
.003* |
a<b, a<c |
|
|
Gastrocnemius |
P1 |
6.59±3.81 |
4.82±3.19 |
3.73±1.64 |
7.982 |
.004* |
c<a |
|
P2 |
8.54±5.97 |
6.53±4.99 |
4.65±3.31 |
12.009 |
.001* |
b<a, c<a |
|
|
Tibialis anterior |
P1 |
0.78±0.35 |
0.83±0.32 |
1.05±0.34 |
14.061 |
.000* |
a<c, b<c |
|
P2 |
0.58±0.40 |
0.61±0.40 |
0.80±0.42 |
8.737 |
.008* |
a<c |
|
A muscle sling is a group of muscles that function together in a movement or exert a combined influence on a movement pattern. Synergists mean muscles working together locally for independent joint movement, whereas muscle slings are interconnected such that a muscle is linked to the origin of an adjacent muscle through a structure in which the contact area becomes a pivot point. Generally speaking, muscle slings are used in multi-joint movement and work together for functional movement rather than contracting independently of each other (Page, Frank & Lardner, 2010). According to Myers (2001), the extensor sling and the flexor sling are muscle slings in the leg. The gluteus maximus, quadriceps, and gastrocnemius constitute the extensor sling, which is involved in extension of the hip and knee and plantar flexion at the ankle. Myers also identified the iliopsoas, hamstring, and tibialis anterior as the flexor sling, which is involved in flexion of the hip and knee and dorsiflexion at the ankle (Myers, 2001). This means that target muscle activation can vary depending on where the CoP is on the sole of the foot. Hence, this study was conducted to investigate the changes in lower extremity muscle activation, CoP, and posture caused by the change in CoP (in the front, middle, and rear of the foot) during squat and to establish scientific evidence based on which an accurate method can be proposed to develop target muscles during training.
This study found that the CoP shifted during a squat in an intended pattern corresponding to the instruction regarding the change in CoP position on the sole of the foot. In the eccentric contraction phase, the CoP was approximately 70% when the instructions called for the front of the foot, approximately 65% for the middle of the foot, and approximately 60% for the rear of the foot (Table 2, p < .05). In the concentric contraction phases, the CoP positions were approximately 73% for the front of the foot, approximately 69% for the middle, and approximately 63% for the rear, again showing a pattern corresponding to the instructions (Table 2, p < .05). The study participants were students in a weight training club who had continuously trained, and the weight was 60% of the 1RM. Thus, it is likely that they were able to shift CoP comfortably during a squat, even with such a heavy weight. However, when a beginner is coached for weight training in a regular gym, closer attention should be paid. In particular, beginners should not try to shift CoP until they have mastered a correct overall posture for squat.
Difference in ROM in the lower extremity joints were examined in relation to the change in CoP. The ROM of the hip was statistically significantly increased with CoP in the rear of the foot compared to in the front (Table 3, p < .05). Applying force to the heel while performing a squat in a correct and stable posture keeps the upper body erect and prevents collapsing. Such an outcome helps the individual perform a deeper squat in a stable way, and consequently, it seems to have resulted in a greater ROM of the hip in study participants. Possibly in support of this interpretation, muscle activation of the erector spinae increased by approximately 20% with CoP in the rear of the foot com- pared to the middle; however, this difference was not statistically significant. In addition, the results of the current study are in line with the findings of Da et al. (2015) that the deeper the individual sat during squat, the more posteriorly the CoP was located.
The ROM of the knee did not show differences across the changes in CoP (Table 3, p >. 05). However, the ankle showed a statistically greater ROM with the CoP in the front of the foot compared to the rear (Table 3, p < .05). The finding regarding the ROM of the knee is believed to be a natural consequence of the fact that the participants were instructed to perform the squat while fixing the feet on the ground. In other words, because the participants maintained a correct squat posture, not lifting the toe area or the heel, the ROM of the knee was not affected by the change in CoP. With regard to the ankle, a greater ROM change occurred with the CoP in the front of the foot compared to the rear. It is speculated that this finding was obtained because the tibia moved posteriorly in the condition in which the CoP was at the rear of the foot, as the ROM of the hip increased and the squat became deeper, which resulted in a smaller dorsiflexion at the ankle.
Regarding the result on the change in lower extremity muscle activation corresponding to the change in CoP, in the eccentric contraction phase the muscle activation of the gastrocnemius was higher by approximately 44% with the CoP in the front of the foot compared to the rear. In the concentric contraction phase, muscle activation was again higher with the CoP in the front of the foot compared to the rear, by approximately 46% (Table 4, p < .05). In contrast, muscle activation of the tibialis anterior was higher with the CoP in the rear of the foot compared to the front, by approximately 26% in the eccentric contraction phase and by approximately 27% in the concentric contraction phase (Table 4, p <. 05). These results are in line with a finding reported by Dionisio et al. (2008) that shifting CoP toward the toe area activated the gastrocnemius and shifting toward the heel activated the tibialis anterior. In the concentric contraction phase, muscle activation of the rectus femoris was higher by approximately 25% with the CoP in the rear of the foot compared to the front, and muscle activation of the gluteus maximus was higher by approximately 7% with the CoP in the front of the foot and by approximately 9% with the CoP in the rear of the foot, compared to the middle (Table 4, p < .05). Myers (2001) reported that the extensor sling in the lower extremities consists of gastrocnemius, quadriceps, and gluteus maximus, and movements occur with the muscles working in coordination. It was reported by Dionisio et al. (2008) as well that the tibialis anterior and the biceps femoris were strongly activated if the weight shifted to the heel, while the gastrocnemius and the quadriceps were strongly activated if the weight shifted to the toe area. However, the current study found that during a squat the gastrocnemius showed greater activation with the CoP in the front of the foot compared to the rear, whereas the rectus femoris showed greater activation with the CoP in the rear of the foot. Also, the finding that the gluteus maximus showed greater activation with the CoP in the rear of the foot compared to the front is contrary to the findings of the previous study. It is speculated that the contrasting result is due to the increase in muscle activation of the gluteus maximus and rectus femoris, because the squat was performed more deeply as ROM of the hip increased by approximately 2% with the CoP in the rear of the foot compared to the front and by approximately 3% compared to the middle. The current study finding is consistent with findings reported by Park, Choi and Kim (2013) and Caterisano et al. (2002) that the deeper the squat position, the higher the level of muscle activation of the gluteus maximus and rectus femoris.
The current findings on muscle activation were based on 60%RM during the squat, which was normalized from the value of muscle activation during half squat without using weights. This can explain why the gluteus maximus alone showed a high level of muscle activation. Bryanton, Kennedy, Carey and Chiu (2012) reported that the load should be increased to strengthen the extensors of the hip, because the heavier the weight used in a squat, the higher the rate of increase in flexor relative muscular effort (RME) in the gluteus maximus. This point is suggested to support the current study results, in which 60%RM was utilized.
It was demonstrated in the current study that during a squat the gastrocnemius showed high muscle activation with the CoP in the front of the foot, whereas the ROM of the hip increased with the CoP in the rear of the foot, and accordingly, muscle activation of the gluteus maximus and rectus femoris increased. Therefore, it should be effective to perform squats with the CoP in the front of the foot if the target muscle is the gastrocnemius, and perform squats with the CoP in the rear of the foot if the target muscles are the gluteus maximus and the quadriceps, i.e., the exercise targets in most cases.
This study investigated the effect of the instructions to shift CoP during squat on ROM, muscle activation, and CoP in the lower extremities. To do so, ROM, CoP, and muscle activation were analyzed while 10 healthy adult men performed squat as they shifted CoP to the front, middle, and rear of the foot following instruction. ROM significantly increased in the hip with the CoP in the rear of the foot compared to the middle, while the ROM of the ankle was significantly higher with the CoP in the front of the foot compared to the rear. The gastrocnemius showed higher muscle activation with the CoP in the front of the foot, and the gluteus maximus, rectus femoris, and tibialis anterior showed higher muscle activation with the CoP in the rear of the foot. Therefore, it is believed that an effective training method in field is to consider different CoP's depending on the target muscle to develop, because the position of CoP influences the level of muscle activation and ROM in the lower extremities during squat.
References
1. Back, S. G. (2016). Effects of Using Convergence Circuit Weight Training on the Blood Lipids and Oxygen-carrying Factors in Middle-aged Women. Journal of the Korea Convergenn Society, 7(6), 267-274.
Crossref
2. Baik, K. & Shin, S. D. (2009). Influence that Exercise Addiction by Leisure Sport Participation Degree Gets in Burn-out. Journal of Sport and Leisure Studies, 38(2), 1271-1283.
Crossref
3. Bak, M. S., Shin, H. S. & Shin, W. (2015). Comparison and analysis of kinetic differences in back squat motions between skilled athletes and ordinary persons. The Korea Journal of Sports Science, 24(1), 1041-1050.
Crossref
4. Beachle, T. R., Earle, R. W. & Wathen, D. (2000). Resistance training. Essentials of strength training and conditioning, 395-425.
Crossref
5. Bryanton, M. A., Kennedy, M. D., Carey, J. P. & Chiu, L. Z. (2012). Effect of squat depth and barbell load on relative muscular effort in squatting. The Journal of Strength & Conditioning Research, 26(10), 2820-2828.
Crossref
Google Scholar
6. Caterisano, A., Moss, R. E., Pellinger, T. K., Woodruff, K., Lewis, V. C., Booth, W. & Khadra, T. (2002). The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. The Journal of Strength & Conditioning Research, 16(3), 428-432.
Crossref
Google Scholar
7. Chae, W. S., Jeong, H. K. & Jang, J. I. (2007). Effect of Different Heel Plates on Muscle Activities During the Squat. Korean Journal of Sport Biomechanics, 17(2), 113-121.
Crossref
Google Scholar
8. Cho, I. H. (2005). The effect of power zone training program on abs/ back and thigh isokinetic muscular function in elite judokas. Journal of Physical Growth and Motor Developmenl, 13(1), 83-89.
Crossref
9. Da, H. K., Lee, J. D. & Kim, K. (2015). Plantar pressures in individuals with normal andpronated foot according to static squat depths. Journal of Physical Therapy Science, 27(9), 2833-2835.
Crossref
Google Scholar
10. De Looze, M. P., Toussaint, H. M., Van Dieen, J. H. & Kemper, H. C. G. (1993). Joint moments and muscle activity in the lower extremities and lower back in lifting and lowering tasks. Journal of Biomechanics, 26(9), 1067-1076.
Crossref
Google Scholar
11. Dionisio, V. C., Almeida, G. L., Duarte, M. & Hirata, R. P. (2008). Kinematic, kinetic and EMG patterns during downward squatting. Journal of Electromyography and Kinesiology, 18(1), 134-143.
Crossref
Google Scholar
12. Escamilla, R. F. (2001). Knee biomechanics of the dynamic squat exercise. Medicine & Science in Sports & Exercise, 33(1), 127-141.
Crossref
Google Scholar
PubMed
13. Fry, A. C., Smith, J. C. & Schilling, B. K. (2003). Effect of knee position on hip and knee torques during the barbell squat. The Journal of Strength & Conditioning Research, 17(4), 629-633.
Crossref
Google Scholar
PubMed
14. Gracovetsky, S. (1997). Linking the spinal engine with the legs. Vleeming (Ed.), Movement, Stability and Low Back Pain-the essential role of the pelvis. Churchill Livingstone.
Crossref
Google Scholar
15. Hermans, H. J., Freriks, B., Merletti, R., Stegeman, D., Blok, J., Rau, G., ... & Hagg, G. (1999). European recommendations for surface electromyography: results of the SENIAM project. Enschede: Roessingh Research and Development BV.
Crossref
Google Scholar
16. Jung, J. H. & Chae, W. S. (2017). The Effect of Exercise Intensity on Muscle Activity and Kinematic Variables of the Lower Extremity during Squat. Korean Journal of Sport Biomechanics, 27(3), 197 -203.
Crossref
Google Scholar
17. Kim, M. S., Seo, I. Y., Jung, G. W., Lee, G. C. & Jung, H. S. (2013). The Effect of the Squat Exercise by Different Baseform on Balance Ability Enhancement in Normal Adult. Journal of Korean Society of Integrative Medicine, 1(3), 63-78.
Crossref
Google Scholar
18. Kim, N. J., Yoo, K. T., An, H. J., Shin, H. J., Koo, J. P., Kim, B. K., ... & Choi, J. H. (2014). The Effects of Balance Exercise on an Unstable Platform and a Stable Platform on Static Balance. Journal of International Academy of Physical Therapy Research, 5(1), 641-646.
Crossref
Google Scholar
19. Lander, J. E., Bates, B. T. & Devita, P. (1986). Biomechanics of the squat exercise using a modified center of mass bar. Medicine and Science in Sport and Exercise, 18, 469-478.
Crossref
Google Scholar
20. Lee, C. H., Nam, K. J. & Kim, J. P. (2013). The difference of motion between Back and Front Squats. The Korea Journal of Sports Science, 22(6), 1557-1569.
Crossref
21. Lee, J. S., Lee, S. D. & Seok, K. H. (2008). The Impacts of Female Swimmers' Participation Motivation on their Leisure Satisfaction. Journal of Sport and Leisure Studies, 32(2), 1195-1203.
Crossref
22. Myers, T. W. (2001). Anatomy Trains. Churchill Livingstone. New York, 137-164.
Crossref
23. Oh, J. H., Kang, S. R., Kwon, T. K. & Min, J. Y. (2015). The Effect on Muscle Activation in the Trunk and Lower Limbs While Squatting with Slope-whole-body Vibration. Korean Journal of Sport Biomechanics, 25(4), 383-391.
Crossref
Google Scholar
24. Page, P., Frank, C. & Lardner, R. (2010). Assessment and treatment of muscle imbalance: the Janda approach. Human kinetics.
Crossref
Google Scholar
25. Park, S. J., Choi, G. R. & Kim, C. K. (2013). Comparison and Analysis of Muscle Acitivities on Angles of Knee Joint during Squat Exercise. Journal of Sport and Leisure Studies, 53(2), 879-887.
Crossref
26. Won, H. H., Kim, M. W., Bae, Y. H. & Kim, Y. J. (2013). A Study on Impact of Squat Exercise on Foot Pressure with different loads. Journal of Fisheries and Marine Sciences Education, 25(4), 891-897.
Crossref
Google Scholar
