Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Jupil Ko
http://dx.doi.org/10.5103/KJSB.2017.27.3.165 Epub 2017 October 15
Abstract
Objective: The Star Excursion Balance Test (SEBT) and Y-Balance Test (YBT) have been commonly applied to measure dynamic postural stability ability. These two tests are utilized interchangeably in various settings. However, they could in fact require different movements to assess dynamic postural stability, as one uses a platform and different measuring techniques than the other. The purpose of this study was to determine if there was a significant difference in the kinematic patterns in physically active population while performing the SEBT and the YBT.
Method: Seventy participants performed in the Anterior (AN), Posteromedial (PM), and Posterolateral (PL) directions of the SEBT and the YBT. The kinematics of hip, knee, and ankle in sagittal plane was calculated and analyzed. Paired-sample t-tests were performed to compare joint angular displacement in the ankle, knee, and hip between the SEBT and the YBT.
Results: Significant differences in angular displacement at the hip, knee, and ankle joints in the sagittal plane between performance on the SEBT and on the YBT were observed.
Conclusion: Clinicians and researchers should not apply these dynamic postural control tasks interchangeably from one task to another. There appear to be kinematic pattern differences between tests in healthy physical active population.
Keywords
Kinematics Postural control Functional performance test Joint angles Healthy population clinical test
The Star Excursion Balance Test (SEBT) is one of the most popular functional performance tests to measure dynamic postural control in a variety of settings (Gribble, Hertel, & Plisky, 2012). A combination of musculoskeletal strength, range of motion (flexibility), and neuromuscular control function is required to perform the SEBT (Plisky, Rauh, Kaminski, & Underwood, 2006). The original format of the SEBT consisted of 8 reach directions including the anterior, anteromedial, medial, posteromedial, posterior, posterolateral, lateral, and anterolateral, but has since been simplified to 3 reach directions (Gray, 1995; Plisky et al., 2006; Plisky et al., 2009). The SEBT showed high reliability with test-retest intra-class correlation ranging from 0.82 to 0.96 and coefficients of variation ranging from 3.0% to 4.6% (Hertel, 2000; Plisky et al., 2006). The SEBT can be easily set up with white athletic tape or measuring tape on any flat floor surface (Olmsted, Carcia, Hertel, & Shultz, 2002).
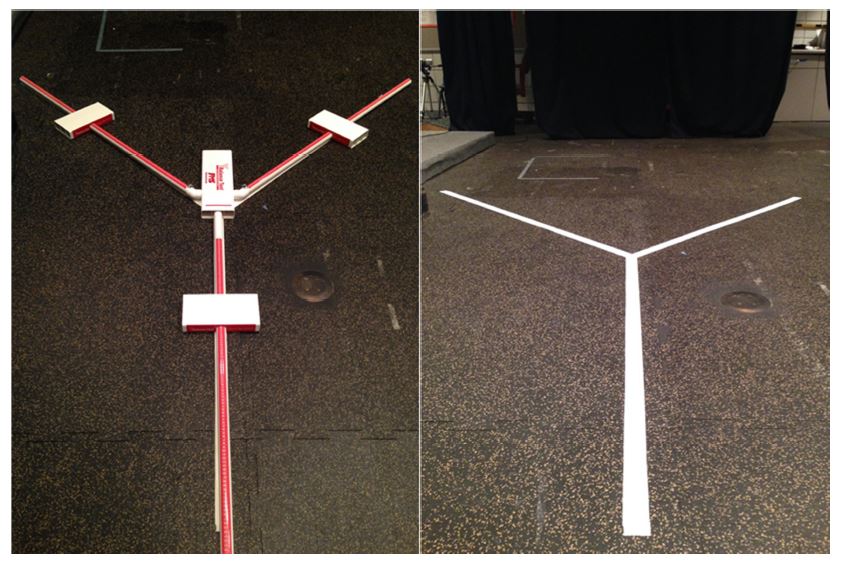
The Y-Balance TestTM (YBT) (Functional Movement.com, Danville, VA) is a modified version of the SEBT to enhance the efficiency of application of the SEBT by using a standardized platform with a moveable measure- ment system. The advantages of the YBT are time efficiency for both the rater to measure and the performer to complete, an established standardized protocol, and ease of reach measurement via a moveable device (Plisky et al., 2009). The YBT is only composed of 3 reach directions including anterior (AN), posteromedial (PM), and posterolateral (PL). A previous study reported excellent inter-rater (0.99~1.00), intra-rater (0.85~0.91), and test-retest reliability, and standard error measure (SEM) among multiple raters on the YBT (Shaffer et al., 2013).
The SEBT and YBT have been commonly applied to assess dynamic postural stability deficits (Gribble et al., 2012; Linens, Ross, Arnold, Gayle, & Pidcoe, 2014; Plisky et al., 2006). In clinical and research settings, these two tests are utilized interchangeably. Although the YBT was developed as a modified version of the SEBT, there is no evidence that indicates that these two tests require a similar task performance and movement strategy. Therefore, the purpose of this study was to determine if there was a significant difference in performance in the kinematic patterns in physically active population while performing the SEBT and the YBT.
We hypothesized that physically active population would have greater angular displacements at the hip, knee, and ankle joints in the sagittal plane on the YBT than on the SEBT.
1. Participants
Tabled data from similar previous studies comparing kinematic patterns in the sagittal plane on the SEBT and the YBT in a healthy population were used to perform a priori sample size was calculated based on means and standard deviations from pilot data from our lab. A total of 13 to 68 per group were required to compare the kinematic patterns for an effect size from 0.05 to 1.2. Therefore, our feasible targeted sample size of 70 participants was set within the established limits of a meaningful sample size for the comparisons of interest.
A total of 70 participants, between 18 to 35 years of age, who participated in physical activity for at least 90 minutes per week, were recruited from the university and community population, via club sports, kinesiology courses, and basic physical education courses at a university (Cho, Kim, Lee, & Lee, 2010). Exclusion criteria included the following: a history of lower extremity surgery or fracture, current signs and symptoms of an acute lower extremity injury, and diagnosis of vestibular disorder, Charcot-Marie Tooth disorder, Ehlers-Danlos disorder, or other nerve or connective tissue disorder (Gribble et al., 2013; Wikstrom & Brown, 2014). All participants were informed of the test procedures and provided an informed consent form during orientation as approved by the local Institutional Review Board.
2. Procedures
A single test session of 30~45 minutes was scheduled in a biomechanics laboratory. Participants completed the demographic questionnaire on injury history and activity. The participants' demographic information was measured including height, mass, gender, and dominant side of limb. Participants were asked the question "With which limb (right or left) would you prefer to kick a ball?" to determine their dominant side (Pietrosimone & Gribble, 2012).
Twenty-nine retro-reflective markers based on the Plug-in-Gait Module (Vicon®, 2002) were applied on the participants' body before they performed the FPTs. Marker trajectories were recorded via an MX-40 ViconTM camera system (Vicon Motion Systems, Oxford, UK), comprised of seven high-speed cameras (240 Hz) using Nexus 2.2.3 software (Vicon Motion Systems, Oxford, UK) with a sampling rate of 120 Hz and mean residual error of ≤ 0.05 mm (Kim et al., 2016; Robinson & Gribble, 2008). The International Society of Biomechanics (ISB) guidelines were applied for setting up the global axis (X-Y-Z) (Wu et al., 2002; Lim & Kwon, 2016).
Participants performed the SEBT and the YBT in a pre-determined counterbalanced order (Figure 1). The test was demonstrated by a single tester before the participants completed 2 practice trials in each of 3 reach directions including AN, PM, and PL. After the practice trials, the participants performed a test trial with the dominant limb in each direction. A trial was classified as failed if the participant removed his or her hands from the hips, did not bring back their reach foot to the starting position, lifted their test foot up or moved their test foot during the test, or kicked the indicator box at the end of the reach to gain more reach distance during the YBT (Plisky et al., 2009). If a trial was classified as failing, the participant was asked to repeat the trial (Gribble, 2003). A single-rater reliability for the SEBT and the YBT was measured prior to data collection. The intra-class correlation coefficient (ICC2,1= 0.89~0.97) and standard error measure (SEM=2.2 cm and 1.6 cm) were excellent.
3. Data reduction and analysis
Means and standard deviations of participants’ demographics was calculated as exploratory descriptive data. All kinematic data were processed through Nexus 2.2.3 (Vicon Motion System, Oxford, England) modeling software. Visual 3D® (C-Motion, Inc., Germantown, MD) biomechanical modeling software was utilized to determine joint kinematics (C-Motion, 2016). Kinematic data at the point of maximum reach for each SEBT and YBT trial were obtained with the test trial for each participant for each direction via Visual 3D® (Fullam, Caulfield, Coughlan, & Delahunt, 2014). To standardize the kinematic data, joint angles were presented as the difference between heel-off to the point of maximum reach by the frame at the heel marker on the reach-foot that was farthest away from the body in the sagittal plane via Vicon 3D® (de la Motte, Arnold, & Ross, 2014; Pozzi, Moffat, & Gutierrez, 2015) The kinematics of hip, knee, and ankle in sagittal plane were calculated and analyzed. Also, sagittal plane angular displacement of the hip, knee, and ankle joint during performance on the 3 reach directions of the SEBT and the YBT were measured (de la Motte et al., 2014; Fullam et al., 2014; Robinson & Gribble, 2008). Joint angular displacement in the ankle, knee, and hip was defined as the difference between the initial and final angular positions of the joint (∆θ = θfinal - θinitial) (Hoch, Gaven, & Weinhandl). The initial angle was determined as the angular position of the ankle, knee, and hip joints when the heel marker on the reaching limb initiated movement to begin the reach. The final joint angle was determined as when the heel marker on the reaching limb was at the point of maximum reach. Cardan angles were used to calculate joint angles in a rotation order of X (flexion and extension), Y (adduction and abduction), and Z (internal and external rotation) for knee and hip joints; and X (dorsiflexion and plantarflexion), Y (inversion and eversion), and Z (internal and external rotation) for ankle joint (Grood & Suntay, 1983).
A 4th order (zero-phase) Butterworth low-pass filter with a 5 Hz cutoff frequency was used to filter the raw marker coordinates for kinematic data (Doherty et al., 2015). The "fill-gap" function in the Vicon Nexus 2.2.3 (Vicon Motion System, Oxford, England) was utilized to fill minor gaps in coordinate positions of reflective markers if a marker was dropped for some frames (Nexus). The fill-gap functions of "rigid body fill", "spline fill", or "pattern fill" were used to fill gaps in the marker path of fewer than 20 frames, depending on which method provided the most similar predicted movement pattern to actual movement pattern (Nexus).
Differences were determined in joint angular displacement in the ankle, knee, and hip in sagittal plane on the SEBT and YBT. Using SPSS Version 22.0 (SPSS Inc, Chicago, IL), paired-sample t-tests were per- formed to compare the reach distance in 3 directions, and joint angular displacement in the ankle, knee, and hip in sagittal planes between on the SEBT and the YBT.
Demographic data are presented (Table 1). Means and standard deviations for joint angular displacements for the hip, knee, and ankle while performing the AN, PM, and PL reach direction of the SEBT and the YBT were reported with powers, p-values, and effect sizes (Cohen's d) (Table 2). The ICC and SEM for each joint angular displacement was between 0.89 to 0.91 and 0.43 to 2.31 (degree), respectively, which has been defined as an acceptable agreement (Chinn, 1991).
|
Group |
Age (yr) |
Height (cm) |
Mass (kg) |
|
Female (35) |
24.75 (±2.22) |
165.71 (±4.23) |
61.20 (±10.55) |
|
Male (35) |
25.45 (±2.12) |
177.31 (±5.14) |
79.94 (±12.56) |
|
Reach direction |
Joint |
Test |
p-value |
Cohen's d |
Power |
|
|
SEBT |
YBT |
|||||
|
AN |
Hip |
9.83±9.22 |
3.47±13.11 |
0.001* |
0.56 |
0.36 |
|
Knee |
43.62±10.71 |
32.70±6.93 |
0.001* |
1.21 |
0.98 |
|
|
Ankle |
21.09±7.52 |
14.13±7.42 |
0.001* |
0.93 |
0.87 |
|
|
PM |
Hip |
54.35±8.98 |
56.13±7.85 |
0.141 |
0.21 |
0.03 |
|
Knee |
46.41±5.90 |
42.77±16.42 |
0.064 |
0.30 |
0.07 |
|
|
Ankle |
14.25±4.92 |
12.18±10.13 |
0.054 |
0.26 |
0.05 |
|
|
PL |
Hip |
46.77±6.19 |
52.46±8.25 |
0.001* |
0.78 |
0.70 |
|
Knee |
19.99±5.61 |
12.87±6.71 |
0.001* |
0.14 |
0.84 |
|
|
Ankle |
8.06±3.96 |
4.82±6.30 |
0.001* |
0.62 |
0.44 |
|
The primary aim of the current study was to investigate the kinematic patterns in the sagittal plane while performing the SEBT and the YBT. The results of the current study partially accept the original hypotheses that physically active population would have greater angular displacements at the hip, knee, and ankle joints in the sagittal plane on the YBT than on the SEBT. All participants exhibited significantly greater angular displacement at the hip, knee, ankle joints in the sagittal plane on the YBT than on the SEBT.
1. Anterior reach direction
The AN reach direction between the SEBT and the YBT, we observed that the participants displayed significantly greater hip flexion, knee flexion, and ankle dorsiflexion angular displacement when performing the SEBT compared with the YBT.
A similar previous study (Fullam et al., 2014) reported opposite results; that is, the healthy population only had significantly less hip flexion angular displacement when performing the AN direction on the SEBT compared with the YBT. Fullam et al. (Fullam et al., 2014) also found that the healthy population showed less knee flexion and ankle dorsiflexion on the SEBT compared with the YBT even though this was not statistically significant. Additionally, a previous study (Robinson & Gribble, 2008) concurred that the hip and knee joint angular displacement in the sagittal plane provided important contributions to performance in selected reach directions of the SEBT.
The results of the current study also revealed that the physically active population required a greater amount of hip flexion, knee flexion, and ankle dorsiflexion angular displacement on the SEBT compared to the YBT. These findings may indicate that the SEBT requires greater sagittal plane angular displacement at the hip, knee, and ankle in the physically active population than the YBT. Therefore, clinicians and researchers should not use these dynamic postural control tasks inter- changeably from one task to another. They appear to be distinct and separate tasks, at least in the AN reach direction.
2. Posteromedial reach direction
There is no significant different kinematic patterns in sagittal-plane angular displacements at hip, knee, and ankle while performing the PM reach direction on the SEBT and YBT. The results from the current study indicate that the physically active population use symmetrically same kinematic patterns on both the SEBT and YBT. Therefore, clinicians and researchers may use the PM reach direction of the SEBT and YBT interchangeably from one task to another.
3. Posterolateral reach direction
The participants exhibited significantly greater hip flexion, knee flexion, and ankle dorsiflexion angular displacements on the YBT compared with the SEBT. To our best knowledge, the current is the first study for comparing angular displacements in the PM reach direction between the SEBT and YBT.
Therefore, it is also suggested that the SEBT and YBT be considered separately as different dynamic postural control tests.
4. Limitations
The authors acknowledge several limitations of this study. Differences in physical ability level between participants may exist. Findings on our recreationally physical active population may not be transferable to other active or non-active populations. The reach distance for each test (performance) could not be measured due to technical issues while data collection session. Therefore, the reach distances need to report in the further study.
The results of the current study indicate there are multiple significant differences in kinematic patterns in the AN and PL reach direction between the SEBT and the YBT. These performance differences may be attributable to the differences in kinematic patterns in the multiple joints we observed. These differences may be modified via rehabilitation interventions and could improve with treatment. Because of the differences in kinematic pattern noted here, clinicians and researchers should be cautious and likely not use the AN and PL reach direction of the SEBT and YBT tests interchangeably.
References
1. C-Motion. (2016). Visual 3D User Guide (Tutorials). Visual3D v5. Retrieved from http://c-motion.com/v3dwiki/index.php?title=Visual3D_Tutorials
Crossref
2. Chinn, S. (1991). Statistics in respiratory medicine. 2. Repeatability and method comparison. Thorax, 46(6), 454-456.
Crossref
Google Scholar
PubMed
3. Cho, J.-H., Kim, K.-H., Lee, H.-D. & Lee, S.-C. (2010). Effects of Rehabilitation Duration on Lower Limb Joints Biomechanics during Drop Landing in Athletes with Functional Ankle Instability. Korean Journal of Sport Biomechanics, 20(4), 395-406.
Crossref
Google Scholar
4. de la Motte, S., Arnold, B. L. & Ross, S. E. (2014). Trunk-rotation differences at maximal reach of the star excursion balance test in participants with chronic ankle instability. Journal of Athletic Training.
Crossref
Google Scholar
5. Doherty, C., Bleakley, C. M., Hertel, J., Caulfield, B., Ryan, J. & Delahunt, E. (2015). Laboratory measures of postural control during the star excursion balance test after acute first-time lateral ankle sprain. Journal of Athletic Training. doi:10.4085/1062-6050-50.1.09
Crossref
Google Scholar
6. Fullam, K., Caulfield, B., Coughlan, G. F. & Delahunt, E. (2014). Kinematic analysis of selected reach directions of the star excursion balance test compared with the y-balance test. Journal of Sport Rehabilitation, 23(1), 27-35. doi:10.1123/jsr.2012-0114
Crossref
Google Scholar
7. Gray, G. W. (1995). Lower Extremity Functional Profile: Wynn Marketing, Incorporated.
Crossref
8. Gribble, P. A. (2003). Considerations for normalizing measures of the star excursion balance test. Measurement in Physical Education and Exercise Science, 7(2), 89-100.
Crossref
Google Scholar
9. Gribble, P. A., Delahunt, E., Bleakley, C., Caulfield, B., Docherty, C. L., Fourchet, F., Wikstrom, E. A. (2013). Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the international ankle consortium. Journal of Orthopaedic & Sports Physical Therapy, 43(8), 585-591. doi:10.2519/ jospt.2013.0303
Crossref
Google Scholar
10. Gribble, P. A., Hertel, J. & Plisky, P. (2012). Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. Journal of Athletic Training, 47(3), 339-357. doi:Doi 10.4085/1062-6050-47.3.08
Crossref
Google Scholar
11. Grood, E. S. & Suntay, W. J. (1983). A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. Journal of Biomechanical Engineering, 105(2), 136-144.
Crossref
Google Scholar
12. Hertel, J. (2000). Intratester and Intertester Reliability During the Star Excursion Balance Tests. Journal of Sport Rehabilitation, 9(PART 2), 104-116.
Crossref
Google Scholar
13. Hoch, M. C., Gaven, S. L. & Weinhandl, J. T. (2016). Kinematic predictors of star excursion balance test performance in individuals with chronic ankle instability. Clinical Biomechanics, 35, 37-41. doi:10.1016/ j.clinbiomech.2016.04.008
Crossref
Google Scholar
14. Kim, J., Cho, H., Han, B., Yoon, S., Park, S., Cho, H., Lee, J. & Lee, H. (2016). Comparison of Biomechanical Characteristics of Rowing Performance between Elite and Non-Elite Scull Rowers. A Pilot Study. Korean Journal of Sport Biomechanics, 26(1), 21-30.
Crossref
Google Scholar
15. Lim, Y. & Kwon, M. (2016). A Comparative Analysis of Biomechanical Factors and Premotor Time of Body Muscles between Elite College and Amateur Baseball Players during the Baseball Batting Motion. Korean Journal of Sport Biomechanics, 26(2), 205-211.
Crossref
16. Linens, S. W., Ross, S. E., Arnold, B. L., Gayle, R. & Pidcoe, P. (2014). Postural-stability tests that identify individuals with chronic ankle instability. Journal of Athletic Training, 49(1), 15-23. doi:10.4085/ 1062-6050-48.6.09
Crossref
Google Scholar
17. Nexus, V. Vicon Nexus User Manual.
Crossref
18. Olmsted, L. C., Carcia, C. R., Hertel, J. & Shultz, S. J. (2002). Efficacy of the Star Excursion Balance Tests in Detecting Reach Deficits in Subjects With Chronic Ankle Instability. Journal of Athletic Training, 37(4), 501-506.
Crossref
Google Scholar
19. Pietrosimone, B. G. & Gribble, P. A. (2012). Chronic ankle instability and corticomotor excitability of the fibularis longus muscle. Journal of Athletic Training, 47(6), 621-626. doi:10.4085/1062-6050-47.6.11
Crossref
Google Scholar
20. Plisky, P., Rauh, M., Kaminski, T. & Underwood, F. (2006). Star excursion balance test as a predictor of lower extremity injury in high school basketball players. The Journal of Orthopaedic and Sports Physical Therapy, 36(12), 911-919.
Crossref
Google Scholar
21. Plisky, P. J., Gorman, P. P., Butler, R. J., Kiesel, K. B., Underwood, F. B. & Elkins, B. (2009). The reliability of an instrumented device for measuring components of the star excursion balance test. North American Journal of Sports Physical Therapy, 4(2), 92-99.
Crossref
Google Scholar
22. Pozzi, F., Moffat, M. & Gutierrez, G. (2015). Neuromuscular control during performance of a dynamic balance task in subjects with and without ankle instability. Int J Sports Phys Ther, 10(4), 520-529.
Crossref
Google Scholar
23. Robinson, R. & Gribble, P. (2008). Kinematic predictors of performance on the Star Excursion Balance Test. Journal of Sport Rehabilitation, 17(4), 347-357.
Crossref
Google Scholar
PubMed
24. Shaffer, S. W., Teyhen, D. S., Lorenson, C. L., Warren, R. L., Koreerat, C. M., Straseske, C. A. & Childs, J. D. (2013). Y-balance test: a reliability study involving multiple raters. Military Medicine, 178(11), 1264-1270. doi:10.7205/MILMED-D-13-00222
Crossref
Google Scholar
25. Vicon®. (2002). Plug-in-Gait modelling instructions. Retrieved from http:// wweb.uta.edu/faculty/ricard/Classes/KINE-5350/PIGManualver1.pdf
Crossref
26. Wikstrom, E. A. & Brown, C. N. (2014). Minimum reporting standards for copers in chronic ankle instability research. Sports Medicine, 44(2), 251-268. doi:10.1007/s40279-013-0111-4
Crossref
Google Scholar
27. Wu, G., Siegler, S., Allard, P., Kirtley, C., Leardini, A. & Rosenbaum, D. (2002). ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion--part I: ankle, hip, and spine. J Biomech, 35(4), 543-548.
Crossref
Google Scholar
