Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Chan-Hee Kim
Joong-Sook Lee
Jeong-Ok Yang
Bom-Jin Lee
Eui-Suk Kim
Kyung-Hee Woo
Jin-Suk Park
http://dx.doi.org/10.5103/KJSB.2017.27.1.59 Epub 2017 April 18
Abstract
Objective: This study investigated the effect of a 16-week upright body exercise program on body balance and plantar pressure balance in elderly women.
Method: The subjects included elderly women in B Metropolitan city who participated in an upright body exercise program twice weekly for 16 weeks. The subjects' physical characteristics (height, weight, body mass index [BMI]), posture balance, and foot plantar pressure were measured before and after the experiment.
Results: The upright body exercise program showed positive changes in posture balance and foot plantar pressure balance in seven elderly women.
Conclusion: The second version of the upright body exercise program improved and may prevent postural imbalance in elderly women. This program could be utilized to improve posture and foot balance in elderly persons.
Keywords
Upright body type exercise program Elderly female Posture balance Foot plantar pressure
South Korea has become an aging society, with the elderly population (65 years and above) accounting for 12.6% of the total population in 2015. In 2018, it is predicted that South Korea will be an aged society, with the elderly accounting for 14.3% of the population. Furthermore, the elderly population is estimated to account for 24.3% in 2030, making South Korea a super-aged society (Korea Statistics, 2015). The average healthy life expectancy in South Korea is currently 73 years, which is 9.3 years shorter than the average life expectancy of 82.3 years (as of 2016) (WHO, 2016). The life expectancies indicate that about 10 years are spent fighting diseases during the elderly years. Medical costs during this period are rapidly becoming a social problem and reduced physical abilities in the elderly decrease their qualities of life (Kim, Lee, & Lee, 2010).
The most prominent problem arising from the decreased independent physical abilities of the elderly is the increase in falls (Regterschot et al., 2014). Falls are the most common problem seen among the elderly, causing small injuries such as bruises and sprains to large injuries such as fractures or dislocations (Rubenstein, 2006). Elderly who experience severe injuries such as pelvic fractures cannot recover their physical abilities (Tinetti, Speechley, & Hinter, 1988). These severe fractures also lead to death in 37% of the elderly (Korea Statistics, 2015). Therefore, falling is a serious issue that influences the satisfaction level of the elderly (WHO, 2008).
Elderly women are especially prone to early decreases in lower limb muscle strength compared to men (Cushnaghan, Janet, & Dieppe, 1991), which increases their relative numbers of musculoskeletal diseases such as arthritis, balance problems, and problems in the main joints such as the pelvic and knee joints (Nevitt et al., 1994). Foot health, which is important for balance, is necessary for weight bearing, gait, and other independent activities. Therefore, maintenance of foot health is impor- tant for the wellness of the main joints (Kim, Kim, & Bang, 2011). Foot problems may cause foot pain and ankle weakness, which decreases physical abilities, such as stair climbing, in the elderly. Furthermore, foot problems negatively affect the maintenance of body balance (Menz, Hylton, & Lord, 2001) and make gait difficult (Dunn et al., 2004).
Foot problems, which are closely related to the overall body balance, cause the body balance to systematically collapse (Eric, 2003). The feet bear the weight of the body. Therefore, problems with the structure of the feet cause body imbalances such as rotation of the trunk or the pelvis. These imbalances cause pain in various parts of the body and affect the chain structure of the knee followed by the waist, pelvis, back, and neck (Cho, 2010). Among the factors that negatively affect balance in the elderly, loss of muscle strength and joint mobility increase the risk of falling. Therefore, maintenance of postural balance through regular exercise is very important for the prevention of injuries (Province et al., 1995).
Upright body exercise is intended to minimize the risk of injuries. Not confined to resistance training, it is useful for the alignment of the musculoskeletal system and also improves balance (Son, 2013; Park, 2015). A study by Kim, Yang, and Lee (2013), which assessed the effects of a 12-week upright body exercise program on 20 female middle school students with scoliosis and Cobb's angles above 10°, reported that the magnitudes of scoliosis and lower back pain were significantly reduced by 36.6% and 54.8%, respectively, after the exercise program.
Many studies on upright body exercise programs have been con- ducted on teenagers. However, there is a lack of studies that target the female elderly. Therefore, this study assessed the effect of a modified version of the upright body exercise program (ver. 2), which has been shown to be effective for improving postural imbalance, on the postural balance foot plantar pressure of female elderly. The goal of this study is to prevent falling and improve the health of elderly women.
1. Subject selection
The study subjects included elderly female residents of B city above 65 years of age. Furthermore, all subjects were diagnosed with body misalignment based on the Physical Activity Promotion System (PAPS) postural evaluation findings (applying to at least one of the categories of tilted cervix, shoulder height, and pelvis height). All 24 selected sub- jects had no communication problems and provided their consent for participation after receiving an explanation of the study objectives and procedures. Ten subjects were excluded from analysis due to incon- sistent participation. Hence, a total of 14 subjects were included in the final results (Table 1).
|
Subject |
Age (years) |
Height (cm) |
Weight (kg) |
BMI (kg/m2) |
|
Exercise group (N = 7) |
64.57 ± |
153.24 ± |
61.79 ± |
26.31 ± |
|
Control group (N = 7) |
64.14 ± |
155.33 ± |
58.29 ± |
26.14 ± |
2. Metrics and analysis method
Prior to the upright body exercise program (Ver. 2), the subject posture and foot plantar pressure were measured in a static standing position.
1) Postural balance measurement
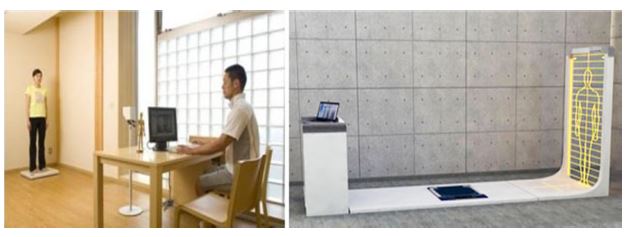
For the measurement of postural balance, images of the participants were taken with the PAPS and analyzed with a whole-body posture analyzer. The Shisei Innovation System (PA200, Japan) can measure whole-body posture from the anterior, posterior, left, and right directions. Furthermore, it can analyze the postural balance, discern the differences in neck/pelvis heights, measure body deviations from the centerline, measure the upper/lower body rotation, and analyze O- and X-shaped lower limbs (Figure 1). In this study, the magnitude of head tilt, shoulder heights, and pelvis heights were measured before and after the exercise and analyzed (Table 2).
|
Measured
items |
Measurement
point |
|
|
Head |
Glabella |
Middle
of the forehead |
|
Pelvis |
Anterior
superior iliac spine (ASIS) |
Front
body projection |
|
Knee |
Front
lower body |
Center
of the patella |
2) Foot plantar pressure measurement
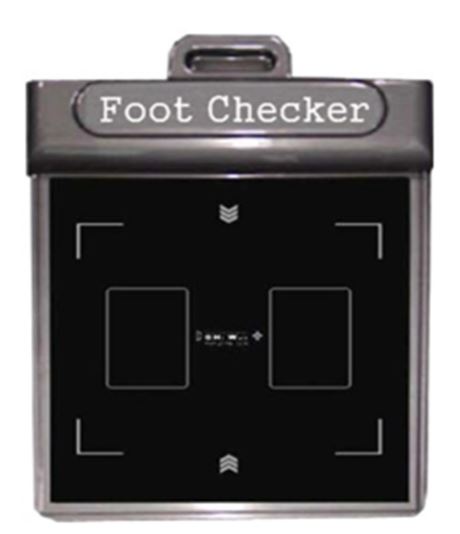
The device to measure foot plantar pressure (GHF-550, GHi. Well, Korea) was designed to measure the foot balance (Figure 3). It contains plantar pressure and balance sensors that show the distribution of plantar pressure step by step. It also quantifies the anterior/posterior and left/right center ratios, turning angle, and the center of the plantar surface of the foot. Therefore, it can be used to analyze the distribution of plantar pressure and the balance. The reference plantar pressure was set to a 50:50 ratio. The metrics and analysis methods are shown in (Table 3), (Figure 2), (Figure 3), and (Figure 4).
|
Subject
measurement |
Measurement
position |
|
Plantar
balance |
Standing
on the whole-foot pressure measurement sensors |
|
Right
foot pressure |
Standing
on the right foot pressure measurement sensors |
|
Left
foot pressure |
Standing
on the left foot pressure measurement sensors |


3. Upright body exercise program (ver. 2.0)
The upright body exercise program was conducted in teams of two. It was developed using body alignment techniques as references (Kim, 2013; Son, 2014; Woo, 2014; Park, 2015) and is effective for the improve- ment of body imbalances. Spine-stabilizing exercises described in a study by Kwon (2011) (transversus abdominis, pelvis joint flexion, vastus medialis, vastus lateralis, and gluteus medius strengthening and flexibility improving exercises) and tension-easing muscle extensions (cervix, pelvis, and lower limbs) by Son, Lee, and Kim (2014) were used as reference. Using these exercises, the warm-up and cool-down exercises were de- veloped with the help of three specialists in related fields. The upright body exercise program was composed of 60-minute long session (10 minutes of warm-up, 40 minutes of main exercise, and 10 minutes of cool-down) and was performed twice weekly over 16 weeks. The inten- sity of the program was scored subjectively by each participant using the Rate of Perceived Exertion (RPE) developed with Borg's scale. The intensities were set to RPE 11~12 for the first 4 weeks, followed by RPE 13~14 for weeks 5~8 and RPE 15~16 for weeks 9~12. The intensity of exercise was determined by RPE ranging between 6 and 20. The RPE described by Borg (1998) is shown in (Table 4).
|
Division |
Workout type |
Duration |
Remarks |
Frequency/Period |
|
Warm-up |
Transverse abdominis rotation, Hip flexion Internal/External oblique side-lying leg lift, Half-squat |
10 min |
• Alternately
conduct all kinds: • 30 sec break between exercises |
Twice weekly for |
|
Main |
Neck exercise, Back exercise, Shoulder exercise, Lumbar build, Pelvis exercise, Hip joint exercise, Abdominis exercise, Knee exercise |
40 min |
• Alternately conduct all exercises: 3 sets of 5~10 repetitions • 30 sec break between sets • 60 sec break between exercises • First set (weeks 1-4) • Second set (weeks 5-10) • Strength: RPE 13~14 |
Twice weekly for |
|
Cool-down |
C-spine, Pelvis, |
10 min |
• Alternately conduct each
exercise: 50 repetitions • 30 sec
break between exercises |
Twice weekly for |
4. Data processing
All collected data were processed using IBM SPSS Statistics for Win- dows, version 23.0. Data analysis was conducted with descriptive statis- tics to determine the averages of the factors in each group as well as their standard deviations. In addition, to prove the homogeneity of the groups prior to the study, independent t-tests were performed for each factor before the experiment. The changes in the factors with confirmed homogeneity before and after the experiment were tested using paired t-tests. The significance level for all data processing was set to α = 0.05.
1. Changes in postural balance before and after upright body exercise program (ver. 2)
The changes in postural alignment before and after the upright body exercise program are shown in (Table 5).
The magnitude of head alignment was determined by measuring the deviation from the centerline of the gravitational force. The experimental group showed a significant 7.29 mm decrease, from 14.71 ± 9.06 mm before exercise to 7.42 ± 7.89 mm after exercise (t = 2.555, p < 0.05). The control group showed a 1.00 mm decrease, from 13.57 ± 10.98 mm before exercise to 12.57 ± 5.62 mm after exercise, which was not a statistically significant change.
There were also significant changes in shoulder alignment in the experimental group, with a significant 7.86 mm decrease from 15.28 ± 6.21 mm before exercise to 7.42 ± 7.89 mm after exercise (t = 3.519, p < 0.05). The control group showed a 0.43 mm decrease from 15.57± 1.71 mm before exercise to 15.14 ± 2.26 mm after exercise, which was not a statistically significant change.
Changes in pelvic alignment in the experimental group showed a significant 10.00 mm decrease, from 14.85 ± 4.01 mm before exercise to 4.85 ± 2.73 mm after exercise (t = 5.728, p < 0.05). The control group showed a 0.29 mm decrease, from 13.57 ± 3.45 mm before exercise to 14.28 ± 3.81 mm after exercise, which was not statistically significant.
|
Group |
Assessment |
Before |
After |
t |
p |
|
Exercise group (N = 7) |
Head |
14.71 ± 9.06 |
7.42 ± 7.89 |
2.555 |
0.043 |
|
Shoulder height |
15.28 ± 6.21 |
7.42 ± 7.89 |
3.519 |
0.013 |
|
|
Pelvic |
14.85 ± 4.01 |
4.85 ± 2.73 |
5.728 |
0.001 |
|
|
Control group (N = 7) |
Head |
13.57 ± 10.98 |
12.57 ± 5.62 |
0.203 |
0.846 |
|
Shoulder-height |
15.57 ± 1.71 |
15.14 ± 2.26 |
0.430 |
0.682 |
|
|
Pelvic |
14.57 ± 3.45 |
14.28 ± 3.81 |
0.154 |
0.883 |
2. Changes in foot plantar pressure balance before and after the upright body exercise program (ver. 2)
The changes in foot plantar pressure balance before and after upright body exercise program (ver. 2) are shown in (Table 6).
The plantar pressure balance of the left foot changed from 44.30 ± 4.71% before exercise to 48.83 ± 2.11% after exercise, while the plan- tar pressure balance of the right foot changed from 55.70 ± 4.71% before exercise to 51.17 ± 4.30% after exercise. Although the plantar pressure ratio of both feet approximated to the ideal 50:50, the changes were not significant. However, the left-right plantar pressure differences decreased significantly, from 13.31 ± 4.30% before exercise to 5.75 ± 4.59% after exercise (t = 4.834, p = 0.002) and approximated to the ideal 50:50 plantar pressure ratio. In the control group, the plantar pres- sure of the left foot changed from 48.88 ± 2.88% before exercise to 47.30 ± 2.12% after exercise, while the plantar pressure of the right foot changed from 52.11 ± 2.88% before exercise to 52.69 ± 2.12% after exercise. The changes in the plantar pressures on both feet were negli- gible. The changes in left-right plantar pressure were also not significant, from 5.50 ± 1.98% before exercise to 13.17 ± 5.26% after exercise.
|
Group |
Assessment |
Before |
After |
t |
p |
|
Exercise group (N = 7) |
Left foot |
44.30 ± 4.71 |
48.83 ± 2.11 |
-2.332 |
0.058 |
|
Right foot |
55.70 ± 4.71 |
51.17 ± 2.11 |
2.332 |
0.058 |
|
|
Difference in values |
13.31 ± 4.30 |
5.75 ± 4.59 |
4.834 |
0.002 |
|
|
Control group (N = 7) |
Left foot |
48.88 ± 2.88 |
47.30 ± 2.12 |
1.105 |
0.311 |
|
Right foot |
52.11 ± 2.88 |
52.69 ± 2.12 |
-1.105 |
0.311 |
|
|
Difference in values |
5.50 ± 1.98 |
13.17 ± 5.26 |
0.395 |
0.706 |
1. Changes in postural balance
Aging and insufficient exercises cause weakened muscle strength and postural imbalance in the elderly. These consequences can not only cause discomforts in daily activities and gait but can also lower life satisfaction by causing respiratory problems such as pneumonia and fractures due to falling (Lord, Murray, Chapman, Munro, & Tiedemann, 2002). In the elderly, musculoskeletal and body changes are usually caused by changes in hormones, reduced physical abilities and weakened musculoskeletal system (Jeon et al., 2005). The most representative change in body is the shortening of the spine due to intervertebral pressure, which causes bending of the back. In addition, the increased curvature of the cervical and thoracic vertebra causes bending of the body towards the front (Frontera et al., 2000). Changes in the vertebra can cause changes in upper/lower length proportions and reduce height. These changes cause postural imbalance as well as changes in the lower limbs such as bending of the legs due to musculoskeletal aging (Lee, 2008).
Arthrogryposis of the knees in the elderly can also cause changes in upper and lower body postures, which lead to postural imbalance (Kim, 2015). Exercise, nutrition programs, and medications are the com- mons treatments for postural imbalance. Among these treatments, exercise is considered the most effective (Kim & Yang, 2009).
Kim (2012) reported improved head and limb positions and posture after a 10-week Pilates exercise program in six female middle school students from S city. Kim (2013) performed an upright body exercise program on 20 female middle school students with Cobb's angles above 10° over 12 weeks, reporting that the program improved body balance. In addition, a study by Son (2014) reported that an upright body exercise program was effective for improving posture, tilted head, tilted shoulders, and tilted pelvis in female high school students with symmetrical imbalances. A study by Woo (2016) reported that an upright body exercise program in patients with intellectual disability effectively improved cervical imbalances such as forward head posture and rounded shoulder into a healthy C-shape. In addition, there were significant improvements in the tilted pelvis. Park (2015) conducted mechanical body-aligning upright body exercises for 12 weeks on male teenagers, reporting that the program effectively improved tilted heads as well as shoulder and pelvis heights.
This study investigated the changes in the postural balance of female elderly following a 16-week upright body exercise program. The changes in tilted head, shoulders, and pelvis were significant in the experi- mental group. Thus, the upright body exercise program was effective in improving tilted head, shoulder, and tilted pelvis as well as returning the postural balance to approximately the center. The results of this study coincide with those of Kim (2013), which reported that an upright body exercise program effectively improved the posture, including the head and the limbs, in female middle school students with body imbalance. A study by Son (2014) reported positive effects on the posture in female high school students with left and right imbalance, and a study by Woo (2013), reported positive effects on the cervical and pelvic tilts in patients with intellectual disabilities. In addition, the results of this study coincide with those of study by Park (2015), which reported that the exercise program effectively improved postural balance in male teenagers with body imbalance. Kim (2012) reported similar results, in which a 10-week Pilates exercise program effectively improved postures, including the head and the upper limbs, in female middle school students. Furthermore, the results of this study coincide with those of study by Han (2004), which reported that a 12-week ver- tebral exercise program effectively improved head and pelvis postures in students with scoliosis, as well as the results of a study by Hwang (2012), which reported positive effects on the postures of the head and the pelvis in adult men.
The results of this and previous studies were analyzed together. The analysis showed that the 16-week upright body exercise program pro- duced similar results to the Pilates and vertebral exercise programs. Therefore, the program developed in this study has similar effects to those of other exercise programs. The 16-week upright body exercise program conducted in this study produced results similar to those of previous studies that incorporated Pilates and vertebral exercise pro- grams. Therefore, it has equivalent effects on improving postural balance. The results of previous studies indicate that the program is effective in female middle school students, female high school students, male adults, and even patients with intellectual disabilities (Kim, 2013; Son, 2014; Woo, 2016; Park, 2015).
Future studies of elderly men with postural imbalance are necessary. The upright body exercise program is expected to have positive effects on balance and muscle strength in this population by aligning their bodies. Expanding and applying the program to elderly with reduced lower limb muscle strength may contribute to improved elderly health.
2. Changes in foot plantar pressure balance
Decreased musculoskeletal functions of the lower limbs in the elderly make normal gait difficult and increase the risk of falls (Liu & So, 2008). The mechanical characteristics of progressive aging tend to reduce the range of motion of the joints, which leads to decreased rounding of the ankle as well as decreased range of motion of inversion, eversion, and rounding of the foot (Vandervoort et al., 1992). Even in elderly without health problems, the range of motion of the ankle may be affected by aging. This decreased ankle range of motion is more pre- valent in elderly women (Jeon, Jeong, & Choi, 2001). Foot problems in the elderly negatively affect the maintenance of body balance and ability to climb stairs due to pain and weakened ankle (Menz, & Lord, 2001). These problems may also cause gait restrictions (Dunn et al., 2004).
Foot balance is closely related to postural balance. Unusual move- ments of the center of mass can cause postural imbalance and verte- bral abnormalities. Furthermore, severe scoliosis causes significant left/ right imbalance, which then affects the plantar pressure (Lim, 2014). In order to improve postural imbalance and plantar pressure imbalance, balance analysis is widely conducted on patients with arthritis as well as patients with foot pain. It is also used to analyze the changes and effects of diverse foot diseases (Park & Lee, 2007).
Cho (2010) reported the positive effects of a Pilates exercise program on improving posture in women in their 20 s. Significant differences in the balances of the left and right plantar pressures were reported. Yoo (2013), conducted foot reflexology and venous relaxation therapy on 33 elderly females, reporting a significantly reduced distribution of plantar pressure as well as positive plantar pressure balance. Lee, Kim, and Lee (2010) reported significant changes in foot imbalance and lumbar angle following lumbar stabilizing exercises in 10 patients with body misalignment. Son (2014), performed a 12-week upright body exercise program in female high school students, reporting that the ratio of both feet approximated the ideal 50%.
The 16-week upright body exercise program in the present study significantly affected plantar pressure balance in elderly women. Sig- nificant changes in the plantar pressure balance of both feet were observed, with the overall plantar pressure balance approximating the ideal 50%.
The upright body exercise program conducted in this study pro- duced results similar to those of Son (2014), which reported improved plantar pressure in female high school students with body imbalance, as well as the results of study by Choi and No (2011), which reported that a six-week PNF exercise program effectively improved plantar pressure balance in patients in their 20 s with misalignment syndrome. In addition, the results coincide with those of study by Cho (2010), which reported that Pilates produced significant changes on the left/right plantar pressure balance in adult women in their 20 s. Yoo (2013), which reported positive effects of foot reflexology and venous relaxation therapy on the plantar pressure balance in elderly women. Finally, a study by Lee, Kim, and Lee (2010) reported significant changes in foot imbalance after lumbar stabilizing exercises, results similar to those of the present study.
The 16-week upright body exercise program produced results similar to those of the reported Pilates, foot reflexology, venous relaxation therapy, and lumbar stabilizing exercises. Therefore, the upright body exercise program effectively improved plantar pressure imbalance. The results are likely due to the positive effects of the upright body exercise program on the balance and the foot posture in the elderly women in the current study. Improvements in postural imbalance correct the movement of the center of mass, which in turn positively affect the left/right plantar pressure balance.
Further studies should assess the effect of an upright body exercise program on the risk of falling, postural imbalance, reduced muscle strength, and muscle imbalance in the elderly, which are the biggest causes of falling in this population. The program may effectively prevent falls and provide gait stability to the elderly.
In summary, the observed improvements in head and shoulder tilt stabilized the vertebra and aligned the upper body to ultimately im- prove postural balance. In addition, changes in the pelvic tilt contributed to lower limb stability and alignment, which in turn improved the plantar pressure balance.
This study analyzed the changes in postural balance and plantar pressure caused by the upright body exercise program. Fourteen elderly female subjects participated in a 60-minute upright body exercise program conducted twice weekly for 16 weeks. After a total of 36 upright body exercise sessions, the following results were obtained.
Firstly, the upright body exercise program effectively improved the postural balances of the head, shoulder, and pelvis in elderly women. These results indicate that the program improved the lower/upper body postural balances and instability of the vertebra and the pelvis. In addition, it is a very effective program for improving lower limb muscle strength. Further studies including subjects of diverse age ranges are necessary to further validate the ability of this program to effectively improve postural imbalance.
Secondly, positive changes in both left and right plantar pressures were observed in elderly women who had completed the upright body exercise program (ver. 2). These results indicate that the exercise program effectively improved their plantar pressure balance. These positive effects on the postural balance show that the program may have directly affected the plantar pressure balance.
Application of the results to elderly exercise programs may improve health in elderly women by improving and preventing musculoskeletal diseases as well as by strengthening lower limb muscles.
References
1. Borg, G. (1998). Brog's perceived exertion and pain scales. Human kinetics.
Google Scholar
2. Cho, D. S. J. (2010). Analysis of basic fitness, body composition and foot balance of women in their twenties according to pilates mate exercise. Unpublished Master's Thesis, Wonkwang University.
Crossref
3. Choi, J. W. & No, H. J. (2011). The Influence of Trunk Rotation Exercise and PNF Exercise on Gait in the Individuals with Malaignment Syndrome. Journal of the Korea Proprioceptive Neuromuscular Facilitation Association, 9(4), 49-55.
4. Cushnaghan, J., McCarth, C. & Dieppe, P. (1994). Taping the petella medially: a new tretment for osteoarthritis of the knee join? British Medical Journal, 308(19), 753-755.
Crossref
Google Scholar
PubMed
5. Dunn, J. E., Link, C. L., Felson, D. T., Crincoli, M. G., Keysor, J. J. & McKinlay, J. B. (2004). Prevalence of foot and ankle conditions in a multiethic community sample of older adults. American Journal of Epidemi- ology, 159(5), 491-498.
Crossref
6. Eric, F. B. (2003). Conditioning for Dance. England: Human Kinetics Publishers.
Crossref
7. Frontera1, W. R., Hughes, V. A., Fielding, R. A., Fiatarone, M. A., Evans, W. J. & Roubenoff, R. (2000). Aging of skeletal muscle: A 12-yr longitudinal study. Journal of Applied Physiology, 88(4), 1321-1326.
Crossref
Google Scholar
8. Han, K. M. (2004). Study on the Spinal-Exercise Program for Improving in Scolisis. Unpublished Master's Thesis, In-ha University.
Crossref
9. Hwang. S. K. (2012). The effects of pilates mat exercises on physical posture and foot balance in male adults. Unpublished Master's Thesis, Myongji University.
Crossref
10. Jeon, M. Y., Jeong, H. C. & Choe, M. A. (2001). A Study on the Elderly Patients Hospitalized by the Fracture from the Fall. Journal of Korean Academy of Nursing, 31(3), 443-453.
Crossref
Google Scholar
11. Jeon, M, Y., Park, E. S., Jeong, B. S., Lee, E. K., Lim, J. S. & Choi, E. S. (2005). The Effects of a Korean Traditional Dance Movement Program in Elderly Women. Journal of Korean Academy of Nursing, 35(7), 1268-1276.
Crossref
Google Scholar
12. Kim, E. S. (2013). Effects of the upright body type exercise program on scoliosis, muscle function and vas in female middle school students. Unpublished Master's Thesis, Silla University.
Crossref
13. Kim, E. S., Yang, J. O. & Lee, J. S. (2013). Utilization of Sport Biomechanics for the Upright Body Type Exercise Program (Centering in Female Middle School Students). Korean Journal of Sport Biomechanics, 23(3), 261-270.
Crossref
Google Scholar
14. Kim, J. Y., Lee, S. G. & Lee, S. K. (2010). The Relationship between Health Behaviors, Health Status, Activities of Daily Living and Health-related Quality of Life in the Elderly. Journal of the Korean Gerontological Society, 30(2), 471-484.
Crossref
15. Kim, M. S. & Yang, S. W. (2009). Effects of Low-intensity Combined Exercise on Body Composition, Blood Lipids, Glucose, and Leptin in Post-menopausal Obese Middle-aged Women. Journal of Sport and Leisure Studies, 38(2), 951-960.
Crossref
16. Kim, S. Y., Kim, S. M. & Bang, S. Y. (2011). Foot Pain and Disability in Community Dwelling Elders. Journal Korean Gerontol Nursing, 13(1), 68-78.
Crossref
17. Kim, Y. J. (2012). The Effect of Pilates Exercise on Body Composition, Posture and Balance of Middle School Girls. Unpublished Master's Thesis, Myongji University.
Crossref
18. Kim, Y. S. (2015). Effects of Thera-Band Yoga on autonomic nervous system and postures in the elderly. Unpublished Master's Thesis, Silla University.
19. Korea, S. (2015). Elderly Statistics. Seoul: Statistics Korea, 2015.
Crossref
20. Kwon, S. S. (2011). Effects of Spinal Stabilization Exercise and Posture Education Program on Vertebra Figures and Inflammation markers, and Fitness Factors in Gymnasts. Unpublished Doctor's Thesis, Korea National Sport University.
Crossref
21. Lee, C. W., Kim, K. T. & Lee, M. C. (2010). The Effects of Using Foot Orthoses and Lumbar Stabilization Exercise that Influence Articular (Lumbosacral & Pelvic Girdle) Angles in Spinal Malalignment Patients with Flatfoot. Journal of Sport and Leisure Studies, 41(2), 748-752.
Crossref
22. Lee, Y. K. (2008). Analysis of lateral body type for elderly women-focused on obesity and deformation of body type. Unpublished Doctor's Thesis, Paichai University.
Crossref
23. Lim, E. J. (2014). The effect of lower limb strengthening exercise and gait training on body balance, Foot pressure and Cobb's angle in high school female scoliosis patients with pelvic malignment syn- drom. Unpublished Master's Thesis, Korea National Sport University.
Crossref
24. Liu, M. R. & So, H. Y. (2008). Effects of Tai Chi Exercise Program on Physical Fitness, Fall related Perception and Health Status in In- stitutionalized Elders. Journal Korean Journal of Korean Academy of Nursing, 38(4), 620-628.
Crossref
Google Scholar
25. Lord, S R., Murray, S. M., Chapman, K., Munro, B. & Tiedeman, A. (2002). Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. The Journal of Gerontology Series A: Biological Sciences and Medical Sciences, 57(8), M539-M543.
Crossref
Google Scholar
26. Menz, H. B. & Lord, S. R. (2001). The contribution of foot problems to mobility impairment and falls in community dwelling older people. Journal of the American Geriatrics Society, 49(12), 1651-1656.
Crossref
Google Scholar
27. Nevitt, M. C, Johnell, O., Black, D. M., Ensrud, K., Genant, H. K. & Cummings, S. R. (1994). Bone mineral density predicts non-spine fractures in very elderly women. Osteoporos International, 4(6), 325-331.
Crossref
Google Scholar
28. Park, J. S. (2015). Effects of Passive Body Alignment Exercise on Regional Alignment and Foot Pressure in Male Adolescent. Unpublished Master's Thesis, Dan Kook University.
Crossref
29. Park, S. B. & Lee, J. S. (2007). Analyses of GRF & Insole Foot-Pressure Distribution: Gait Patterns and Type of Trekking Boots. Korean Journal of Sport Biomechanics, 17(4), 190-200.
Crossref
Google Scholar
30. Province, M. A., Hadley, E. C., Hornbrook, M. C., Lipsitz L. A., Miller, J. P., Mulrow, C. D., Ory, M. G., Sattin, R. W., Tinetti, M. E. & Wolf, S. L. (1995). The effects of exercise on falls in elderly patients, The Journal of the American Medical Association, 273(17), 1341-1347.
Crossref
Google Scholar
31. Regterschot, G. R. H., Folkersma, M., Zhang, W., Baldus, H., Stevens, M. & Zijlstra, W. (2014). Sensitivity of sensor-based sit-to-stand peak power to the effects of training leg strength, leg power and balance in older adults. Gait & Posture, 39(1), 303-307.
Crossref
Google Scholar
32. Rubenstein, L. Z. (2006). Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing, 35 Supply 2, ii37-ii41.
Crossref
Google Scholar
PubMed
33. Son, N. Y. (2014). Effects of the upright body type exercise program on postures and foot balance in female high school students. Unpublished Master's Thesis, Silla University.
Crossref
Google Scholar
34. Son, N. Y., Lee, J. S. & Kim. J. H. (2014). Effects of the Upright Body Type Exercise Program on Postures and Foot Balance in Female High School Students. Korea Journal of Sport Biomechanics, 24(1), 75-83.
Crossref
35. Tinetti, M., E., Speechley, M. & Ginter, S. F. (1988). Risk factor for falls among elderly persons living in the communite. New England Journal of Medicine, 31(9), 1701-1707.
Crossref
Google Scholar
36. Vandervoort, A. A., Chesworth, B. M., Cunningham, D. A., Paterson, D. H., Rechnitzer, P. A. & Koval, J. J. (1992). An outcome measure to quantify passive stiffness of the ankle. Canada Journal Public Health, 83(2), 19-23.
Crossref
Google Scholar
37. WHO (2008). WHO global report on falls prevention in older age. World. Health Organization: World Health Organization.
Crossref
Google Scholar
38. WHO (2016). World Health Statistics 2016: Monitoring health for the SDGs.
Crossref
Google Scholar
PubMed
39. Woo, K. H. (2014). Effects of the Upright Body Type Exercise Program on Autonomic Nervous System, Balance, VAS in Female Middle School Student. Unpublished Master's Thesis, Silla University.
Crossref
40. Woo, K. H. (2016). Effects of the upright body type exercise program on posture, Muscle Strength of leg, lung capacity and depression in people with mental illness. Unpublished Doctor's Thesis, Silla University.
Crossref
41. Yoo, S. J. (2013). The Effects of Foot Reflexology and Venous Relaxation Massage on Female Elderly Persons' Plantar Pressure, Balance, and Psychological Stability. Unpublished Doctor's Thesis, Daegu University.
Crossref
