Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Junhyeong Kwon
Sunghe Ha
Inje Lee
Se Jong Kim
Sae Yong Lee
http://dx.doi.org/10.5103/KJAB.2024.34.3.133 Epub 2024 September 26
Abstract
Objective: Neuromuscular training may often result in an incomplete improvement of biomechanical risk factors associated with non-contact ACL injury. This study aimed to investigate the effects of reactive neuromuscular training (RNT) on dynamic postural control of the lower extremity during single-leg drop landing (SLDL) in comparison with conventional neuromuscular training (CNT).
Method: Twenty-eight recreational female athletes were randomized to a CNT group (n=15) or a RNT group (n=13). All participants performed SLDL for three-dimensional motion analysis before and after CNT and RNT. The kinematic variable was calculated from before 50 milliseconds (ms) to after 100 ms initial contact: joint angle (degree). The kinetic variable was calculated from initial contact to after 100 ms: internal net joint moment (Nm/kg). Time series curve for normalized data was represented for group means and associated 95% confidence intervals. Effect sizes using Cohen's d was also calculated.
Results: In within-group differences, the CNT group showed decreased knee flexion angle (0~100% of the task) and decreased knee valgus angle (0~50% of the task) after the intervention, whereas the RNT group showed increased hip flexion angle (0~14% of the task), decreased hip adduction angle (0~100% of the task), and decreased knee valgus angle (0~100% of the task) after the intervention. In between-group differences, the RNT group exhibited more hip flexion angle (0~49, 61~91% of the task), more knee flexion angle (0~100% of the task), and less knee valgus angle (0~55% of the task) than the CNT group.
Conclusion: These findings suggest that both training intervention programs modified dynamic posture of the hip and knee during SLDL. Therefore, combining a neuromuscular training program with RNT technique would be more efficient for future injury prevention efforts.
Keywords
Neuromuscular training Reactive neuromuscular training Anterior cruciate ligament injury Dynamic postural control Biomechanics
Anterior cruciate ligament (ACL) injury may result in long-term disability such as post-traumatic osteoarthritis and can have associated socio-economic problems (Montalvo et al., 2019; Sugimoto, Myer, Foss & Hewett, 2015). In terms of gen- der differences, studies have consistently shown that female athletes have a higher non-contact ACL injury rate than males in sports (Arendt & Dick, 1995; DeHaven & Lintner, 1986). Especially, during sport-related movements that require jump-landing and/or sudden changes in direction, the females are up to six times more likely to suffer a non-contact ACL injury compared with males (Arendt, Agel & Dick, 1999; Harmon & Ireland, 2000). These results are because women have bio- mechanical and neuromuscular characteristics that different from men in the lower extremity when performing common athletic tasks (Henry & Kaeding, 2001; Lephart, Ferris, Riemann, Myers & Fu, 2002). Thus, the main issue for preventing non-contact ACL injury in female athletes is to address these neuromuscular and biomechanical characteristics.
Abnormal neuromuscular control during dynamic activities can lead to altered lower extremity biomechanics including hip adduction and internal rotation, knee flexion, abduction and external rotation (Hewett, Myer & Ford, 2006; Mehl et al., 2018). This neuromuscular control deficits result in poor postural control during jump-landing tasks and, it may be one determinant of the ACL injury mechanism in female athletes (Hewett, Ford, Hoogenboom & Myer, 2010; Hewett et al., 2005; Lopes et al., 2018; Malinzak, Colby, Kirkendall, Yu & Garrett, 2001). Thus, the ability to execute the proper dynamic posture of the hip and knee joint during landing is crucial to reducing the risk of injury, and this ability needs to be honed in ACL injury prevention programs (Nessler, Denney & Sampley, 2017).
Neuromuscular training which improves neuromuscular control of the lower extremity biomechanics during a landing task may be required to adapt the motor program for the maintenance and accomplishment of postural control (Brown, Palmieri-Smith & McLean, 2014; Horak, Nashner & Diener, 1990; Myer, Ford, Brent & Hewett, 2006; Pfile et al., 2013; Riemann & Lephart, 2002). However, some studies reported that the biomechanical variables associated with non-contact ACL injury are not as sensitive to neuromuscular-based train- ing (Brown et al., 2014; Chappell & Limpisvasti, 2008; Greska, Nelson Cortes, Van Lunen & Oñate, 2012; Lephart et al., 2005; Lopes et al., 2018; Myer, Ford, McLean & Hewett, 2006; Pappas et al., 2015). The reason for the conflicting findings could be a lack of consideration during conventional neuromuscular training (CNT) for stimulating appropriate stabilizing reactions allowing for the control of high-risk joint translation during landing tasks. Furthermore, no studies have described the types of neuromuscular training conducted to improve neuro- muscular control in lower extremity biomechanics during landing.
The concept of reactive neuromuscular training (RNT), first introduced by Voight and Cook, is to train individuals to re- cognize good movement by themselves through an external force (Cook, Burton & Fields, 1999; Voight & Cook, 1996). In other words, this training approach aims to restore altered neuromuscular control systems by giving athletes information on high-risk movements in advance (Hoogenboom, Voight & Prentice, 2014; Lephart, Pincivero, Giraido & Fu, 1997). Some studies support the use of RNT in muscular imbalance (Cook et al., 1999), balance ability (Kim, 2012) and knee abduction moments (Pittman, 2013). Nevertheless, evidence is limited on improvements in dynamic posture and prevention of non-contact ACL injury brought about by RNT. Therefore, the effectiveness of RNT on dynamic postural control should be investigated.
Thus, our study aimed to determine the extent to which RNT could successfully modify the three-dimensional bio- mechanics of the hip and knee joints following single-leg drop landing (SLDL) in female athletes and compared the findings with those of CNT. We hypothesized that there are differences between RNT and CNT in their effects on the kinetic and kine- matic patterns of the hip and knee joints during SLDL.
1. Study design
We followed a randomized controlled trial design with intervention blinding. The independent variables were group (RNT and CNT) and time (preintervention, postintervention), and the dependent variables were three-dimensional kine- matics (joint angle) and kinetics (net internal joint moment) of the hip and knee during SLDL. Study approval was obtained from the Institutional Review Board of Yonsei University and written informed consent was obtained from all participants before participation (7001988-202003-HR-812-02).
2. Participants
We recruited 32 healthy female recreational athletes from the university and the surrounding community. A recreational athlete was defined as an individual who engages in sports or exercise involving unilateral landing tasks (e.g., soccer, basket- ball, volleyball, and so on) one to three times per week or who previously participated in such sports at the varsity level in high school and competed at least once a month. All partici- pants were randomized to a CNT group (n=15) or an RNT group (n=15). We excluded a participant if she (1) did not meet the criterion for an age of between 20 and 30 years old, (2) did not meet the recreational athlete criterion, (3) had a surgery or injury in the lower extremity within 6 months be- fore the study, (4) had cardiovascular, respiratory, neurological, or other disease that prevented her from engaging in sub- maximal effort in sports activity, (5) had ever suffered an ACL injury, or (6) had participated in a formal injury prevention training within 6 months before the study. Throughout the study, participants could continue their aerobic or sports activities before they participated in this study but could not initiate new aerobic.
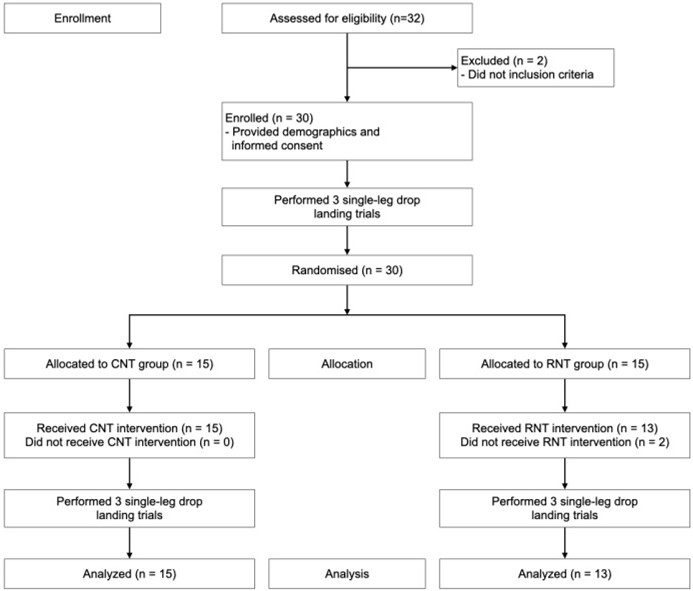
3. Procedure
The procedures are outlined in Figure 1. After enrollment, three-dimensional joint angles and moments of the hip and knee were measured using an eight-camera motion analysis system (Vicon Motion Systems, Oxford Metric Ltd., UK) at a sampling rate of 200 Hz. Ground reaction force data were also collected using an embedded force platform (AMTI, Watertown, MA, USA) with a sampling rate of 2,000 Hz. We time-synchronized the force plates to the motion analysis system to determine initial contact during SLDL.
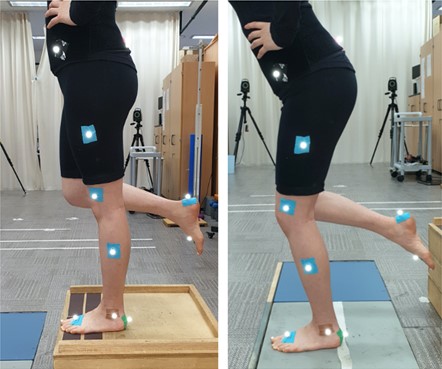
We attached 16 retroreflective markers (11 mm) to land- marks of the lower extremities (bilaterally: anterior superior iliac spine, posterior superior iliac spine, lateral thigh, lateral knee, lateral tibia, lateral malleolus, second metatarsal head, and calcaneus). We initiated motion analysis by asking the participants to stand in a neutral position (the anatomical position) for 5 s, which was captured by placing their feet on the two force plates to set the standard angle. Then, they performed an SLDL on their dominant leg, which is defined as their preferred kicking leg (Brophy, Silvers, Gonzales & Mandelbaum, 2010) (Figure 2). Next, the participants were asked to stand with their non-dominant leg on a 30 cm-high platform and to drop from the platform and land onto the middle of a force plate using the dominant leg (Teng, Kong & Leong, 2017). An assistant researcher demonstrated the testing sequence. We allowed the participants to go through several practice trials so they could correctly execute the required movements. During the test, the tasks were repeated until data from three successful trials were achieved. A trial was successful when the participant stepped off the platform without any jump action and adopted a stable landing posture without losing balance. After 6-week training intervention, all partici- pants completed a postintervention assessment.
4. Training intervention
The participants were divided into two groups. One group underwent a CNT program that was based on previously pub- lished studies on improvements of potential biomechanical risk factors of ACL injury (Hopper, Haff, Joyce, Lloyd & Haff, 2017; Lopes et al., 2018) (Table 1). The second group under- went a RNT program that was a modification of the CNT program and included the RNT technique, which involves educating the participants regarding lower extremity valgus motion through external resistance with an elastic band (Table 2). During the session, they should exert every effort to main- tain and return to the neutral position of the lower extremity by resisting the valgus force applied by an instructor. The in- structor gave verbal guidance like "resist the force I'm applying" or "try to keep your posture" so that the participants could perform the movement correctly. The instructor controlled the resistance level so as not to apply excessive feedback to the participants, cause functional failure, or cause the participants pain or discomfort during the training. For both training groups, the training intervention lasted 6 weeks and consisted of three sessions per week of not more than 20 min each, as described previously (Hewett et al., 2006; Pappas et al., 2015; Sadoghi, von Keudell & Vavken, 2012). The sessions were con- ducted on non-consecutive days, for a total of 18 training sessions. Both groups were instructed to perform a dynamic warm-up before each session.
|
Exercise |
Set |
Time or |
Rest |
|
Phase 1 (for weeks 1 through 2) |
|
|
|
|
Double leg squat and push off |
2 |
12 reps |
60 |
|
Double leg squat jump |
1 |
8 reps |
|
|
Double leg jumps and stick |
2 |
6 reps |
|
|
Forward barrier jump |
2 |
15 sec |
|
|
Broad jump (forward, vertical) |
1 |
8 reps |
|
|
Phase 2 (for weeks 3 through 4) |
|
|
|
|
Double-leg squat jump |
1 |
8 reps |
60 |
|
Single leg push-off |
1 |
6 reps |
|
|
Single leg squat |
1 |
6 reps |
|
|
Crossover hop and stick |
2 |
6 reps |
|
|
Single leg hops and stick |
2 |
6 reps |
|
|
Forward barrier hops |
2 |
15 sec |
|
|
Phase 3 (for weeks 5 through 6) |
|
|
|
|
Double-leg squat jump |
1 |
6 reps |
60 |
|
Single leg squat jump |
1 |
4 reps |
|
|
Broad jump (forward, vertical) |
2 |
6 reps |
|
|
Broad hops (forward, vertical) |
2 |
5 reps |
|
|
Single leg hops and stick |
2 |
5 reps |
|
|
Crossover hop and stick |
2 |
6 reps |
|
Exercise |
Set |
Time or repetition |
Rest |
|
Phase 1 (for weeks 1 through 2) |
|
|
|
|
Double leg squat and push off (with RNT
technique) |
2 |
12 reps |
60 |
|
Double leg squat jump (with RNT
technique) |
1 |
8 reps |
|
|
Double leg jumps and stick (with RNT
technique) |
2 |
6 reps |
|
|
Forward barrier jump |
2 |
15 sec |
|
|
Broad jump (forward, vertical) (with RNT
technique) |
1 |
8 reps |
|
|
Phase 2 (for weeks 3 through 4) |
|
|
|
|
Double-leg squat jump (with RNT
technique) |
1 |
8 reps |
60 |
|
Single leg push-off (with RNT technique) |
1 |
6 reps |
|
|
Single leg squat (with RNT technique) |
1 |
6 reps |
|
|
Crossover hop and stick (right to left)
(with RNT technique) |
2 |
6 reps |
|
|
Single leg hops and stick (with RNT
technique) |
2 |
6 reps |
|
|
Forward barrier hops |
2 |
15 sec |
|
|
Phase 3 (for weeks 5 through 6) |
|
|
|
|
Double-leg squat jump (with RNT
technique) |
1 |
6 reps |
60 |
|
Single leg squat jump (with RNT
technique) |
1 |
4 reps |
|
|
Broad jump (forward, vertical) (with RNT
technique) |
2 |
6 reps |
|
|
Broad hops (forward, vertical) (with RNT
technique) |
2 |
5 reps |
|
|
Single leg hops and stick (with RNT
technique) |
2 |
5 reps |
|
|
Crossover hop and stick (right to left)
(with RNT technique) |
2 |
6 reps |
5. Data processing and statistical analysis
Each participant's joint angles and net internal joint moments of the hip and knee were computed and analyzed in the sagittal, frontal, and transverse planes during preintervention and postintervention SLDL. Non-contact ACL injuries likely occur in the first 100 milliseconds (ms) after initial ground contact (Dai et al., 2018; Koga et al., 2010). Therefore, joint angles (degree) were analyzed over a 150 ms time interval from 50 ms before initial contact to 100 ms after initial contact. Net internal joint moments (Nm/kg) were also analyzed over a 100 ms time interval from initial contact to 100 ms after IC. Initial contact was defined as the point where the force plate data reached more than 10 N. The time intervals were reduced to 100 frames so that each frame represented 1% of the task. All outcome measures were analyzed as an average of three trials.
We used RStudio (RStudio Inc, US) to plot the time series curve for normalized kinematic and kinetic data across 100% of the SLDL. Group means and associated 95% confidence intervals (CIs) were represented for the entire task. Areas where the CIs for at least 3 consecutive percentage points did not overlap between the curve were considered differences. We calculated the mean differences and associated standard devi- ations for the identified increments (Weltman, 2013). Addition- ally, we calculated Cohen's d effect sizes for all dependent vari- ables using mean differences and associated pooled standard deviations to interpret within- and between-group differences after the intervention (Slater & Hart, 2016). Effect sizes will be interpreted as small (< 0.40), moderate (0.40~0.80), or large (> 0.80) (Cohen, 1992). Independent-sample t-test was used to assess group differences in primary demographics.
There were no statistically significant differences between CNT and RNT groups in demography characteristics: age (CNT: 23.7±2.9 yr., RNT: 25.9±2.8 yr., p = .059), height (CNT: 166.7±6.5 cm, RNT: 162.4±5.0 cm, p = .063), and body mass (CNT: 61.2±7.5 kg, RNT: 56.1±9.1 kg, p = .114). RNT group of this study was analyzed only 13 except 2 participants who dis- continued intervention.
1. Within-group difference
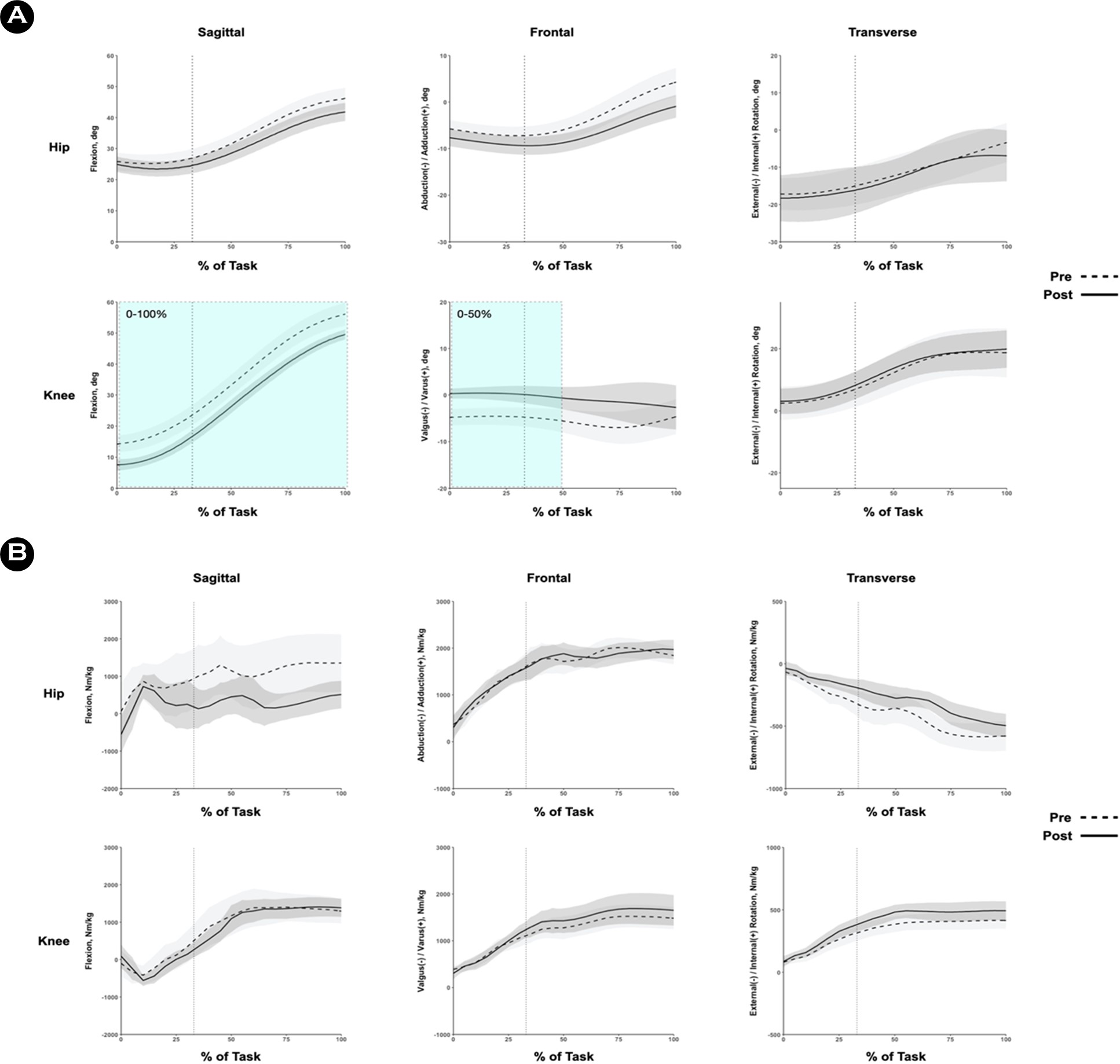
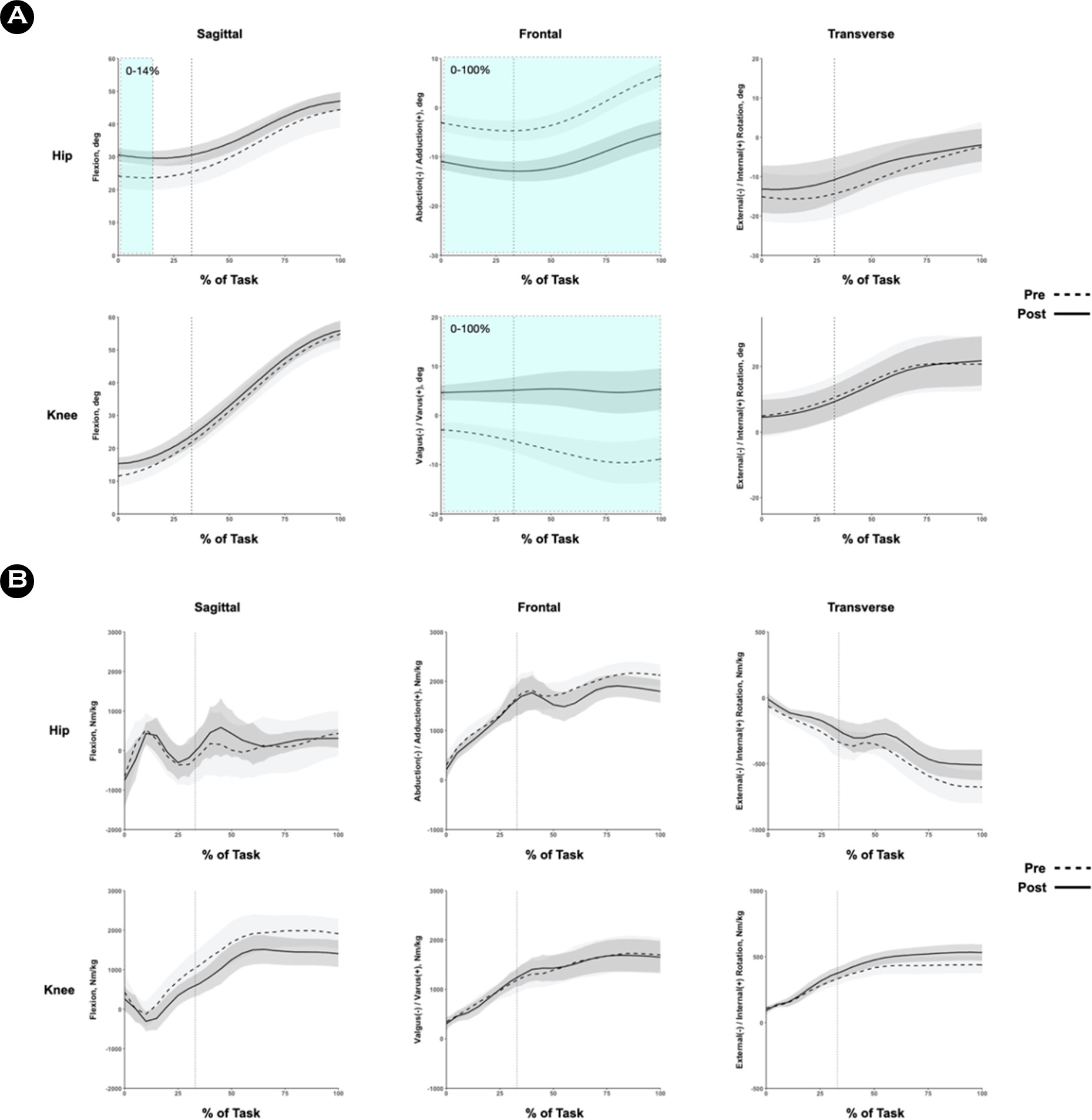
At postintervention, both groups demonstrated significant within-group improvement in kinematics. In the CNT group, the knee flexion angle decreased at 0~100% of the task (mean difference = 7.05°; Cohen d range = -1.27 to -0.88; Figure 3A). In addition, the knee valgus angle decreased at 0~50% of the task (mean difference = 4.92°; Cohen d range = 0.99 to 1.43; Figure 3A). In the RNT group, the hip flexion angle increased at 0~14% of the task (mean difference = 6.21°; Cohen d range = 0.87 to 0.94; Figure 4A). The hip adduction angle decreased at 0~100% of the task (mean difference = 9.19°; Cohen d range = -2.67 to -2.07; Figure 4A). Similarly, the knee valgus angle decreased at 0~100% of the task (mean difference = 11.75°; Cohen d range = 1.69 to 2.61; Figure 4A). The differences in all kinetic outcomes were not significant (Figure 3B and 4B).
2. Between-group difference
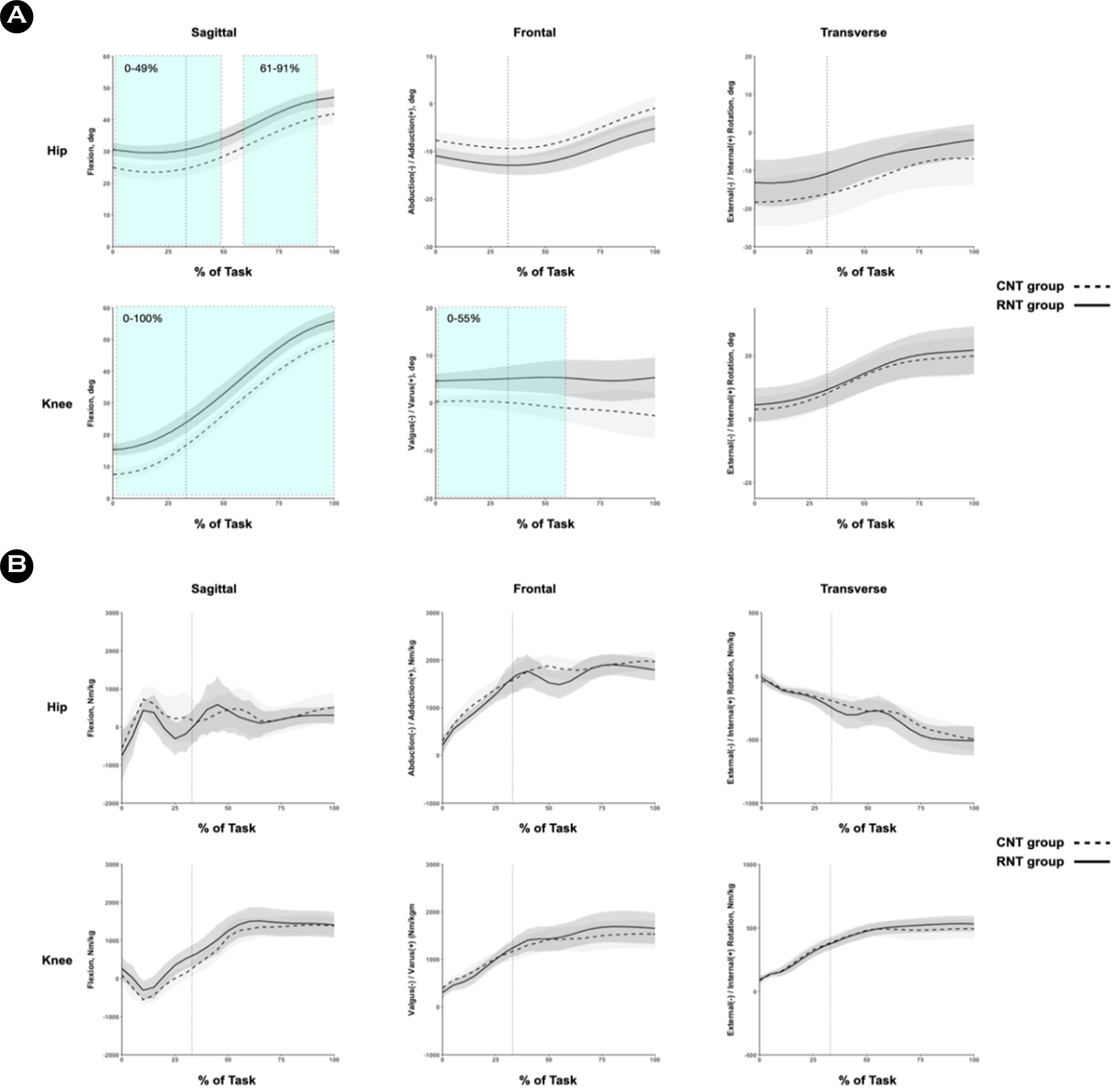
The RNT group exhibited more hip flexion angle at 0~49% (mean difference = 5.94°; Cohen d range = -1.61 to -1.07) and 61~91% (mean difference = 5.68°; Cohen d range = -1.26 to -1.09) of the task, respectively (Figure 5A), compared with the CNT group. Similarly, compared with the CNT group, the RNT group showed more knee flexion angle at 0~100% of the task (mean difference = 7.1°; Cohen d range = -2.28 to -1.06) and less knee valgus angle at 0~55% (mean difference = 5°; Cohen d range = -1.55 to -0.95; Figure 5A). We found no significant differences in all kinetic outcomes (Figure 5B).
Essentially, both training programs in our study focused on the correction of movement patterns that may increase injury risk during SLDL. After the intervention, both groups exhibited less knee valgus angle than before the intervention. Specif- ically, the RNT group showed a much smaller knee valgus angle than before the intervention during the entire landing task. Although significant differences in the CNT group were observed mainly before initial contact, this finding is similar to those of other studies on the effect of neuromuscular training on biomechanics in the lower extremity (Hopper et al., 2017; Myer, Ford, McLean, et al., 2006).
A significant decrease in hip adduction and knee valgus angle was observed in the RNT group from the beginning of the pre-landing phase (before initial contact) to after initial contact. This may be attributed to the RNT technique, which enabled the RNT group to maintain the hip-abducted and knee-adducted posture throughout the training sessions. Due to this external force applied to their knee, the RNT group seems to have utilized their feed-forward motor control system to perform reduced adduction angles of the hip from the pre-landing phase. On the other hand, we found no significant change in the frontal plane motion of the hip within the CNT group. We presume that the participants in the CNT group performed the movement primarily by using the knee control strategy. In fact, we found that the CNT group showed only decreased knee valgus motion after the training intervention program they experienced. This perspective corroborates with the findings of a previous study suggesting that valgus collapse of the lower extremity during single leg tasks is governed primarily by knee motion rather than by the hip and ankle (Myer, Ford, McLean, et al., 2006). However, although the RNT group showed a significant change in both the hip and knee motion, this does not necessarily indicate that the CNT program is inferior to the RNT program in improving postural control ability. There is a possibility that the largely decreased hip adduction angle in the RNT group may be due to lateral pelvic drop or trunk lean towards the stance leg. This ipsilateral pelvic drop or trunk lean can cause a shift in center of mass towards the stance leg, increasing hip abduction motion (Chijimatsu et al., 2020). Unfortunately, due to the limitations of measuring instruments, we were unable to investigate pelvic and trunk kinematics. Future research investigating the effects of RNT on pelvic and trunk in compared to CNT is required.
The participants in the CNT group showed a decreased knee flexion angle after the intervention throughout the entire phase from pre-landing to post-initial contact. Although this finding is in direct contrast to those of previous studies (Brown et al., 2014; Chappell & Limpisvasti, 2008; Lephart et al., 2005), we hypothesize that this would be due to postural adaptation to single leg-focused training. Typically, discrepancies may occur in sagittal plane motion due to the distinct biomechanical demands of each type of landing task (Brown et al., 2014). For instance, unilateral landing is characterized by a decrease in knee flexion at touchdown (Weinhandl, Joshi & O'Connor, 2010). This motion may be a compensatory strategy for decel- erating the body efficiently and absorbing the impact forces of landing by reducing the moment arm of the body center of mass in the sagittal plane (Pappas, Hagins, Sheikhzadeh, Nordin & Rose, 2007). The CNT program used in our study mainly consisted of exercise elements related to single leg movement. In addition, the participants performed the CNT program with no verbal instruction regarding soft landing techniques which can lead to a deep knee flexion motion. Further research is needed to confirm our evaluations.
At postintervention, the RNT group performed SLDL with less knee abduction angle than the CNT group during the entire pre-landing and early stance phases of the task. This finding can be interpreted in two contexts. The first interpret- ation is that the RNT technique elicited a reactive movement through reflex pathways, thus the RNT group were able to control their knee valgus posture in the frontal plane better than the CNT group. This premise agrees with the findings of a previous study (Dhaher, Tsoumanis & Rymer, 2003). This reflex response may be important in preserving knee joint stability by activating regional muscles and inducing wide- spread muscle activation throughout the lower extremity. In this context, the RNT program may have induced reflex activity in the knee muscles, thereby facilitating the ability to prepare for an anti-valgus posture from the pre-landing phase. Further electromyographic studies are needed. The second interpret- ation is that the RNT group showed 'excessively' adducted knee posture due to the RNT technique while the CNT group showed a frontal plane neutral posture of the knee at post- intervention. We speculated that a valgus force through the RNT technique with a resistance band caused externally rotated foot position at landing. In fact, foot rotation positions can influence knee valgus/varus motion during unilateral landing task (Teng et al., 2017). However, only the hip and knee joints were examined in our study, which should be addressed in future studies.
The RNT group further showed a greater hip and knee flexion motion compared with the CNT group during SLDL, specifically showing a significant increase in the knee flexion motion after the 6 week-training intervention. This may indicate that the RNT participants had relatively softer landings than the CNT group. Increased sagittal plane motion during the landing task may reduce strain on the ACL (Beynnon et al., 1995; Hirokawa, Solomonow, Lu, Lou & D'Ambrosia, 1992). In this context, the RNT may be relatively better than the CNT in improving neuromuscular control in sagittal plane motion and in reducing non-contact ACL injury risk during single-leg landing. However, in terms of within-group differences, the RNT group showed no significant change in knee flexion and no other significant differences in kinetics. Thus, future research is required to describe further the effects of RNT on dynamic hip and knee postures in the sagittal plane.
Our study has several limitations. First, only one type of landing task was examined. Most other studies that investi- gated the effects of neuromuscular training on landing bio- mechanics evaluated a variety of landing-related tasks. This is a significant limitation of this study since non-contact ACL injury occurs during several athletic movements in sports. Therefore, understanding the effects of reactive neuromuscular training program on movement biomechanics during these types of tasks is important. Second, the RNT program in this study only involved knee valgus perturbation for about 20 min. Future studies are needed to identify the effects of hip joint perturbation and training durations of less than 20 min to get the maximal effect with minimal effort for non-contact ACL injury prevention.
Both the 6-week CNT and RNT programs for recreational female athletes resulted in postural control change in the hip and knee during single-leg drop landing. In particular, the RNT program was more efficient over the same amount of time. The potential risk of non-contact ACL injury can be decreased in recreational female athletes by adopting an injury preven- tion strategy that combines a neuromuscular training program with the RNT technique.
References
1. Arendt, E. & Dick, R. (1995). Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. The American Journal of Sports Medicine, 23(6), 694-701.
Google Scholar
2. Arendt, E. A., Agel, J. & Dick, R. (1999). Anterior cruciate liga- ment injury patterns among collegiate men and women. Journal of Athletic Training, 34(2), 86.
Google Scholar
3. Beynnon, B. D., Fleming, B. C., Johnson, R. J., Nichols, C. E., Renström, P. A. & Pope, M. H. (1995). Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. The American Journal of Sports Medicine, 23(1), 24-34.
Google Scholar
4. Brophy, R., Silvers, H. J., Gonzales, T. & Mandelbaum, B. R. (2010). Gender influences: the role of leg dominance in ACL injury among soccer players. British Journal of Sports Medicine, 44(10), 694-697.
Google Scholar
5. Brown, T. N., Palmieri-Smith, R. M. & McLean, S. G. (2014). Comparative adaptations of lower limb biomechanics during unilateral and bilateral landings after different neuromuscular-based ACL injury prevention protocols. The Journal of Strength & Conditioning Research, 28(10), 2859-2871.
Google Scholar
6. Chappell, J. D. & Limpisvasti, O. (2008). Effect of a neuro- muscular training program on the kinetics and kinematics of jumping tasks. The American Journal of Sports Medicine, 36(6), 1081-1086.
Google Scholar
7. Chijimatsu, M., Ishida, T., Yamanaka, M., Taniguchi, S., Ueno, R., Ikuta, R., Samukawa, M., Ino, T., Kasahara, S. & Tohyama, H. (2020). Landing instructions focused on pelvic and trunk lateral tilt decrease the knee abduction moment during a single-leg drop vertical jump. Physical Therapy in Sport, 46, 226-233.
Google Scholar
8. Cohen, J. (1992). Quantitative methods in psychology: A power primer. Psychological Bulletin, 112, 1155-1159.
Google Scholar
9. Cook, G., Burton, L. & Fields, K. (1999). Reactive neuromuscular training for the anterior cruciate ligament-deficient knee: a case report. Journal of Athletic Training, 34(2), 194.
Google Scholar
10. Dai, B., Cook, R. F., Meyer, E. A., Sciascia, Y., Hinshaw, T. J., Wang, C. & Zhu, Q. (2018). The effect of a secondary cognitive task on landing mechanics and jump performance. Sports Biomechanics, 17(2), 192-205.
Google Scholar
11. DeHaven, K. E. & Lintner, D. M. (1986). Athletic injuries: com- parison by age, sport, and gender. The American Journal of Sports Medicine, 14(3), 218-224.
Google Scholar
12. Dhaher, Y. Y., Tsoumanis, A. & Rymer, W. Z. (2003). Reflex muscle contractions can be elicited by valgus positional perturbations of the human knee. Journal of Biomechanics, 36(2), 199-209.
Google Scholar
13. Greska, E. K., Nelson Cortes, D., Van Lunen, B. L. & Oñate, J. A. (2012). A feedback inclusive neuromuscular training pro- gram alters frontal plane kinematics. Journal of Strength and Conditioning Research, 26(6), 1609.
Google Scholar
14. Harmon, K. G. & Ireland, M. L. (2000). Gender differences in noncontact anterior cruciate ligament injuries. Clinics in Sports Medicine, 19(2), 287-302.
Google Scholar
15. Henry, J. & Kaeding, C. (2001). Neuromuscular differences between male and female athletes. Current Women's Health Reports, 1(3), 241-244.
Google Scholar
16. Hewett, T. E., Ford, K. R., Hoogenboom, B. J. & Myer, G. D. (2010). Understanding and preventing acl injuries: current biomechanical and epidemiologic considerations-update 2010. North American Journal of Sports Physical Therapy: NAJSPT, 5(4), 234.
Google Scholar
17. Hewett, T. E., Myer, G. D. & Ford, K. R. (2006). Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. The American Journal of Sports Medicine, 34(2), 299-311.
Google Scholar
18. Hewett, T. E., Myer, G. D., Ford, K. R., Heidt Jr, R. S., Colosimo, A. J., McLean, S. G., van den Bogert, A. J., Paterno, M. V. & Succop, P. (2005). Biomechanical measures of neuro- muscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. The American Journal of Sports Medicine, 33(4), 492-501.
Google Scholar
19. Hirokawa, S., Solomonow, M., Lu, Y., Lou, Z. P. & D'Ambrosia, R. (1992). Anterior-posterior and rotational displacement of the tibia elicited by quadriceps contraction. The American Journal of Sports Medicine, 20(3), 299-306.
Google Scholar
20. Hoogenboom, B. J., Voight, M. L. & Prentice, W. E. (2014). Musculoskeletal Interventions 3/E: McGraw Hill Profes- sional.
21. Hopper, A. J., Haff, E. E., Joyce, C., Lloyd, R. S. & Haff, G. G. (2017). Neuromuscular training improves lower extremity biomechanics associated with knee injury during landing in 11~13 year old female netball athletes: A randomized control study. Frontiers in Physiology, 8, 883.
Google Scholar
22. Horak, F., Nashner, L. & Diener, H. (1990). Postural strategies associated with somatosensory and vestibular loss. Experi- mental Brain Research, 82(1), 167-177.
Google Scholar
23. Kim, W. W. (2012). Effects of Reactive Neuromuscular Training and Baps-Trampoline Training on Balance Ability and Isokinetic Muscle Function. The Official Journal of the Korean Academy of Kinesiology, 14(2), 127-136.
Google Scholar
24. Koga, H., Nakamae, A., Shima, Y., Iwasa, J., Myklebust, G., Engebretsen, L., Bahr, R. & Krosshaug, T. (2010). Mech- anisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. The American Journal of Sports Medicine, 38(11), 2218-2225.
Google Scholar
25. Lephart, S. M., Abt, J., Ferris, C., Sell, T., Nagai, T., Myers, J. & Irrgang, J. (2005). Neuromuscular and biomechanical char- acteristic changes in high school athletes: a plyometric versus basic resistance program. British Journal of Sports Medicine, 39(12), 932-938.
Google Scholar
26. Lephart, S. M., Ferris, C. M., Riemann, B. L., Myers, J. B. & Fu, F. H. (2002). Gender differences in strength and lower extremity kinematics during landing. Clinical Orthopaedics and Related Research (1976-2007), 401, 162-169.
Google Scholar
27. Lephart, S. M., Pincivero, D. M., Giraido, J. L. & Fu, F. H. (1997). The role of proprioception in the management and rehabilitation of athletic injuries. The American Journal of Sports Medicine, 25(1), 130-137.
Google Scholar
28. Lopes, T. J. A., Simic, M., Myer, G. D., Ford, K. R., Hewett, T. E. & Pappas, E. (2018). The effects of injury prevention pro- grams on the biomechanics of landing tasks: a systematic review with meta-analysis. The American Journal of Sports Medicine, 46(6), 1492-1499.
Google Scholar
29. Malinzak, R. A., Colby, S. M., Kirkendall, D. T., Yu, B. & Garrett, W. E. (2001). A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clinical Biomechanics, 16(5), 438-445.
Google Scholar
30. Mehl, J., Diermeier, T., Herbst, E., Imhoff, A. B., Stoffels, T., Zantop, T., Petersen, W. & Achtnich, A. (2018). Evidence-based concepts for prevention of knee and ACL injuries. 2017 guidelines of the ligament committee of the German Knee Society (DKG). Archives of Orthopaedic and Trauma Surgery, 138(1), 51-61.
Google Scholar
31. Montalvo, A. M., Schneider, D. K., Yut, L., Webster, K. E., Beynnon, B., Kocher, M. S. & Myer, G. D. (2019). "What's my risk of sustaining an ACL injury while playing sports?" A systematic review with meta-analysis. British Journal of Sports Medicine, 53(16), 1003-1012.
Google Scholar
32. Myer, G. D., Ford, K. R., Brent, J. L. & Hewett, T. E. (2006). The effects of plyometric vs. dynamic stabilization and balance training on power, balance, and landing force in female athletes. Journal of Strength and Conditioning Research, 20(2), 345.
Google Scholar
33. Myer, G. D., Ford, K. R., McLean, S. G. & Hewett, T. E. (2006). The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. The American Journal of Sports Medicine, 34(3), 445-455.
Google Scholar
34. Nessler, T., Denney, L. & Sampley, J. (2017). ACL injury pre- vention: what does research tell us? Current Reviews in Musculoskeletal Medicine, 10(3), 281-288.
Google Scholar
35. Pappas, E., Hagins, M., Sheikhzadeh, A., Nordin, M. & Rose, D. (2007). Biomechanical differences between unilateral and bilateral landings from a jump: gender differences. Clinical Journal of Sport Medicine, 17(4), 263-268.
Google Scholar
36. Pappas, E., Nightingale, E. J., Simic, M., Ford, K. R., Hewett, T. E. & Myer, G. D. (2015). Do exercises used in injury pre- vention programmes modify cutting task biomechanics? A systematic review with meta-analysis. British Journal of Sports Medicine, 49(10), 673-680.
Google Scholar
37. Pfile, K. R., Hart, J. M., Herman, D. C., Hertel, J., Kerrigan, D. C. & Ingersoll, C. D. (2013). Different exercise training inter- ventions and drop-landing biomechanics in high school female athletes. Journal of Athletic Training, 48(4), 450-462.
Google Scholar
38. Pittman, M. (2013). Biomechanical Differences at the knee after two types of hip abductor training: Traditional vs. Reactive neuromuscular training: California State University, Fullerton.
Google Scholar
39. Riemann, B. L. & Lephart, S. M. (2002). The sensorimotor system, part II: the role of proprioception in motor control and functional joint stability. Journal of Athletic Training, 37(1), 80.
Google Scholar
40. Sadoghi, P., von Keudell, A. & Vavken, P. (2012). Effectiveness of anterior cruciate ligament injury prevention training programs. JBJS, 94(9), 769-776.
Google Scholar
41. Slater, L. V. & Hart, J. M. (2016). The influence of knee align- ment on lower extremity kinetics during squats. Journal of Electromyography and Kinesiology, 31, 96-103.
Google Scholar
42. Sugimoto, D., Myer, G. D., Foss, K. D. B. & Hewett, T. E. (2015). Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: meta-analysis and sub- group analysis. British Journal of Sports Medicine, 49(5), 282-289.
Google Scholar
43. Teng, P., Kong, P. & Leong, K. (2017). Effects of foot rotation positions on knee valgus during single-leg drop landing: Implications for ACL injury risk reduction. The Knee, 24(3), 547-554.
Google Scholar
44. Voight, M. L. & Cook, G. (1996). Clinical application of closed kinetic chain exercise. Journal of Sport Rehabilitation, 5(1), 25-44.
Google Scholar
45. Weinhandl, J. T., Joshi, M. & O'Connor, K. M. (2010). Gender comparisons between unilateral and bilateral landings. Journal of Applied Biomechanics, 26(4), 444-453.
Google Scholar
46. Weltman, A. (2013). Jogging Biomechanics after Exercise in Individuals with ACL-Reconstructed Knees.
Google Scholar
