Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Jae-Hu Jung
Woen-Sik Chae
http://dx.doi.org/10.5103/KJAB.2024.34.3.125 Epub 2024 September 26
Abstract
Objective: The purpose of this research was to analyze the effects of applying functional electrical stimulation (FES) on function of the ankle joint and gait ability of the elderly.
Method: In this research, 12 male participants over 65 who have no musculoskeletal disorder were recruited as research subjects. For this research, in order to analyze the function of the ankle joint and gait ability of the elderly depending on the application of FES, all subjects were tested WF (with FES) and WOF (without FES) in random order and 72-hour of resting was assigned between the conditions. For WF condition, 30-minute of FES treatment (frequency 90 Hz, pulse width 400 µs, on-off ratio 1:1) on ankle joint basal flexor muscle was implemented, and afterwards, Isokinetic muscle function on the ankle joint and gait ability were conducted for each condition.
Results: The result showed that the maximum strength of ankle joint basal flexion motion WF statistically significantly increased compared to WOF. The single support ratio of gait motion WF statistically significantly decreased compared to that WOF.
Conclusion: Thus, applying FES is considered to mitigate the functional decline of basal flexor of the elderly, and furthermore, it is considered to have positive effect on improvement of gait ability.
Keywords
Functional electrical stimulation Muscle function Gait ability Elderly
낮은 출산율과 늘어난 기대수명으로 인한 평균 연령의 증가는 전 세계적으로 고령화를 가속시키고 있다(Kontis et al., 2017; Mathers, Stevens, Boerma, White & Tobias, 2015). 고령 사회 진입에 따른 노인 인구의 증가는 만성질환 발병률을 높일 뿐만 아니라 노화에 따른 신체 기능 저하로 인해 노인들의 삶의 질을 크게 저하시킨다(Kirkwood, Trede, de Souza Moreira, Kirkwood & Pereira, 2011). 노화에 따른 신체 기능의 저하는 균형 조절 능력을 감소시키고 보행과 같은 기능적 운동 능력의 장애를 유발시키는 원인이 된다(Campbell, Spears & Borrie, 1990; Tinetti & Ginter, 1988). 특히 대부분의 노인들에게 나타나는 균형 조절 능력의 감소는 보행 중 낙상의 위험성을 증가시킨다(Gillespie et al., 2003; Miller, 2002). 이러한 노인들의 균형 조절 능력 및 보행 기능의 저하는 신체 중심 이동에 필요한 추진력 발휘와 충격력 제어에 있어서 중요한 역할을 담당하는 발목관절의 불안정성에 의해 발생된다(Ha, Kim & Han, 2013). 발목관절의 불안정성은 근력 저하와 관절가동범위의 감소로 인해 유발되며, 이러한 결과로 인해 보행 동작 시 보폭시간과 보폭길이의 가변성이 증가되고 보행속도가 감소된다(Aggio et al., 2016; Callisaya et al., 2011; Cromwell & Newton, 2004; Jeon, 2001).
노인들에게서 나타나는 보행 기능 저하는 근감소증, 근력 감소와 유의한 관련성이 있는 것으로 판단된다(Carr, 2021). 발목관절의 근기능이 저하된 노인들은 관절 주변 근육과 건의 연결부가 약해지는 양상을 보이며(Karamanidis & Arampatzis, 2011), 이로 인해 근력 발휘를 위한 반응시간 지연, 균형 조절 능력 감소와 같은 운동 수행력의 저하가 나타난다(Klass, Baudry & Duchateau, 2011). 또한 낙상 발생의 원인과 관계되는 신체의 전후 방향에 대한 안정성 및 균형성 유지는 전경골근과 내측비복근의 교대 활성에 의해 이루어지게 되는데, 하퇴 근력이 저하되거나 발목관절의 유연성이 감소될 경우 낙상 발생 위험성이 높아지게 된다(Almeida, Carvalho & Talis, 2006; Menz, Morris & Lord, 2006). 이처럼 노화에 따른 보행 기능 장애를 완화하기 위해서는 발목을 비롯한 하지관절 주위 근육들의 근력과 근기능을 향상시켜야 한다(Kim, 2012; Cooper, Taylor & Feller, 2005; Mir, Hadian, Talebian & Nasseri, 2008).
현재 노인들의 발목관절을 비롯한 하지 근골격계 기능 저하를 치료하기 위한 방법으로 약물요법, 물리치료 및 재활운동 등의 보존적 요법이 사용되고 있다. 하지만 보존적 요법을 통한 일반적인 근력 및 근기능 향상 방법은 퇴행성 변화로 약해져 있는 발목관절의 근기능 회복에 부정적인 영향을 미치고, 노인들의 신체활동 기피 현상을 초래해 하퇴 근육의 기능을 약화시킨다(An & Won, 2012; Gardner, Robertson & Campbell, 2000). 최근 이러한 문제점을 해결하기 위해 노인들의 관절 및 근육 조직에 부담을 주지 않고 원하는 부위의 근력 및 근기능을 향상시킬 수 있는 기능적 전기자극(functional electrical stimulation, FES) 치료법이 널리 보급되고 있다. 근육의 인위적인 수축과 이완을 유도하는 FES 치료는 정상적인 신경 지배를 받고 있는 감각신경과 운동신경을 자극하여 수의적 운동보다 더 강한 근육활동을 발생시킴으로써, 근육량 증가, 근력 및 근지구력 향상, 근위축 방지 등에 효과가 있는 것으로 밝혀졌다(Pekindil, Sarikaya, Birtane, Pekindil & Salan, 2001). 이러한 FES 치료는 신체활동이나 근육의 수의적인 수축에 의한 근력 강화가 어려운 노인들의 근육 위축 및 근감소증을 예방하기 위한 목적으로 활용되고 있다(Lin & Yan, 2011).
FES 치료의 임상적 효과와 관련된 선행연구들을 살펴보면, 근섬유의 모세혈관 증가 및 혈관 생성 촉진(Chekanov et al., 2002), 혈류량 증가(Kaplan, Czyrny, Fung, Unsworth & Hirsh, 2002), 골격근의 근력 증가(Granat, Ferguson, Andrews & Delargy, 1993), 신경근 연접 부위의 운동단위 증가(Petersen, Taylor & Gandevia, 2002; Vanderthommen et al., 2002), 손상된 중추신경의 기능 개선(Chae, Fang, Walker & Pourmehdi, 2001; Crameri, Weston, Climstein, Davis & Sutton, 2002) 등의 효과가 있다고 보고되었다. 또한 FES 치료는 하지 근골격계 손상 환자들의 재활 치료 측면에서 부상 부위의 통증 완화 및 근위축 감소를 위한 운동 방법으로도 권장되고 있다. 실제 하지관절 근기능이 저하된 노인들을 대상으로 FES 치료와 재활운동프로그램을 적용한 결과, 무릎관절의 움직임에 직접적으로 관여하는 대퇴사두근을 비롯한 하지 근육의 근력 회복 및 근위축 예방, 통증 완화에 도움이 된다고 밝혀졌다(Bily, Trimmel, Mödlin, Kaider & Kern, 2008; Romero, Sanford, Schroeder & Fahey, 1981; Talbot, Gaines, Ling & Metter, 2003). 또한 퇴행성 관절염 환자들을 대상으로 FES 치료를 실시한 연구에서도 외측광근의 두께 증가, 무릎관절의 신전 토크 향상, 근육의 긴강도 및 경직도 감소, 관절 및 근육의 기능 제한 완화 등 FES 치료에 따른 긍정적인 효과가 나타났다고 보고하였다(Vaz et al., 2013).
FES 치료에 관한 다수의 선행연구에서 밝혀진 바와 같이, FES에 의한 근수축은 노인들의 근골격계 기능을 증진시키는데 효과적인 것으로 판단된다. 또한 근력 향상 측면에서 FES에 의한 근수축은 수의적 근수축과 유사한 효과를 기대할 수 있다(Maffiuletti et al., 2006). 하지만 FES 치료에 관한 기존의 연구들은 FES 적용에 따른 근위축 감소와 근력 증강과 같은 재활 효과 검증, 부상 부위의 통증 완화에 관한 임상적 연구에 국한되어 있으며, 인체의 운동 기능적 특성과 관련된 연구는 미흡한 실정이다. 특히 노인들을 대상으로 FES 적용 유무에 따른 발목관절의 등속성 근기능 및 보행 능력을 분석한 연구는 전무한 실정이다. 따라서 본 연구의 목적은 FES 적용이 노인의 발목관절 근기능과 보행 능력에 미치는 영향을 분석하는데 있다. 이를 위해 노인들을 대상으로 FES 적용 유무에 따라 발목관절에 대한 등속성 근기능 검사 및 보행 능력 검사를 실시하였다.
1. 연구대상자
본 연구에서는 인체 근골격계에 이상이 없고 주 사용발이 오른발인 65세 이상 남성 12명(연령 73.7±5.9세, 신장 166.9±5.2 cm, 체중 68.8±6.6 kg)을 연구대상자로 선정하였다.
2. 실험장비
1) 기능적 전기자극(functional electrical stimulation, FES) 치료기
본 연구에서는 FES 적용을 위해 기능적 전기자극 치료기(MICROSTIM2, SEJINMT, Korea)를 활용하였으며, 주파수 가용 범위는 1~99 Hz, 펄스 지속시간의 가용 범위는 10~700 μs이다. FES 적용 방법은 기능적 전기자극 치료기와 연결된 전극을 해당 근육의 근위부와 원위부에 각각 부착한 후 정적인 상태에서 전기자극을 적용하였다(Gaines, Metter & Talbot, 2004).
2) 등속성 근기능 검사
등속성 근기능 검사는 등속성 운동기기(Humac Norm, CSMI, USA)를 사용하여 피험자의 우측 발목관절 운동에 대한 최대근력과 근지구력을 측정하였다(Figure 1). 피험자가 검사기기에 대한 생소함이나 거부감을 줄이고 최대 능력을 발휘할 수 있도록 검사에 앞서 3회의 연습을 실시하였으며, 각 측정항목 사이에는 3분의 휴식시간을 부여하였다. 발목관절의 저측굴곡 및 배측굴곡 동작 시 하지를 제외한 다른 신체부위에 불필요한 힘이 작용하지 않도록 하기 위해 측정기기에 연결된 벨트로 피험자의 복부와 대퇴부를 고정하였다. 또한 등속성 운동기기와 발목관절의 회전축이 서로 일치하도록 조정하였으며, 힘점이 되는 발목관절의 밑쪽에 패드가 위치하도록 길이를 조절하였다. 본 검사에서 최대근력은 60°/sec에서 3회 반복, 근지구력은 180°/sec에서 15회 반복 실시하였으며, 이때 발목관절의 가동 범위는 60°로 설정하였다.

3) 보행 능력 검사
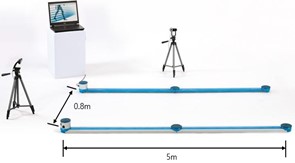
보행 능력 검사는 OPTOgait 시스템(OPTOgait, Microgate Inc., Italy)을 사용하여 보행 동작에 대한 분석 변인을 측정하였다(Figure 2). OPTOgait 시스템은 1 m 길이의 송수신 막대를 길이 5 m, 폭 0.8 m로 나란히 2줄로 설치하였으며, LED 다이오드가 지면으로부터 3 mm 높이에 1 cm 간격으로 각 송수신 막대 속에 배치되었다. 본 실험에서는 보행 동작 시 OPTOgait 1.6.4.0 버전의 소프트웨어(Microgate Inc., Italy)를 이용하여 자료를 수집하였으며, 자료 수집 시 샘플링 주파수는 1,000 Hz로 설정하였다.
3. 실험절차
본 연구의 피험자들은 실험에 들어가기 전 피로를 유발시킬 수 있는 강도 높은 신체활동을 금지하였으며, 실험에 앞서 10분간 가볍게 워밍업을 실시하였다. 본 실험에서는 FES 적용 유무에 따른 노인들의 발목관절 근기능과 보행 능력을 분석하기 위해 모든 피험자를 대상으로 FES 적용 유무에 따른 FES 적용(with FES, WF) 조건과 FES 미적용(without FES, WOF) 조건을 적용하였다. 이때 각 조건의 실시 순서에 의한 효과를 배제하기 위해 피험자별 2가지 조건의 적용 순서를 무선할당(randomization) 방식을 통해 선정하였으며, 각각의 실험 조건 적용 간 근피로에 의한 영향을 배제하기 위해 약 72시간의 휴식시간을 부여하였다. FES 적용 조건에서는 FES 치료기와 연결된 4개의 전극을 양측 비복근의 근위부와 원위부에 각각 부착한 후 정적인 상태에서 발목관절 저측굴곡근에 대해 30분간 FES 치료(frequency 90 Hz, pulse width 400 μs, on-off ratio 1:1)를 실시하였다(Gaines et al., 2004). FES 치료 시 전극 부착 부위는 Van Abbema et al. (2015)의 연구 결과를 참고하여 보행 능력에 큰 영향을 미치는 근육인 발목관절 저측굴곡근으로 선정하였다. 이후 각 조건에 대해 발목관절에 대한 등속성 근기능 검사와 보행 능력 검사를 실시하였다.
4. 자료분석
1) 등속성 근기능 검사
등속성 운동기기(Humac Norm, CSMI, USA)를 사용하여 우측 하퇴 근육의 저측굴곡 및 배측굴곡 동작에 대한 최대근력, 근지구력 자료를 각각 분석하였다. 최대근력은 부하속도 60°/sec에서 3회 반복 시 최대값, 근지구력은 부하속도 180°/sec에서 15회 반복 시 전체 일량을 활용하였으며, 각 피험자의 체중으로 표준화하였다.
2) 보행 능력 검사
본 연구에서는 보행 동작 분석을 위해 OPTOgait 1.6.4.0 버전의 소프트웨어(Microgate Inc., Italy)를 이용하였다. OPTOgait 시스템에서 보행 동작 시, 지면과 나란히 배치된 두 막대 사이를 발이 지나갈 때 LED 다이오드 간의 송수신을 차단하여 사물의 크기 및 거리가 감지되며 시공간적 매개변수가 자동으로 산출되어진다. 모든 자료는 OPTOgait 1.6.4.0 버전의 소프트웨어(Microgate Inc., Italy)를 이용하여 수집하였으며, 보행 동작에 대한 보폭 소요시간(step time), 보폭(step length), 보행속도(speed), 분당 보폭 수(cadence), 보행 주기에서 한발이 지면에 접촉하고 있는 시간의 비율인 한발 지지구간(single support) 비율, 보행 주기에서 양발이 지면에 접촉하고 있는 시간의 비율인 양발 지지구간(double support) 비율을 산출하였다.
5. 통계처리
본 연구에서는 노인들의 발목관절 등속성 근기능 검사 및 보행 능력 검사 시 FES 적용 유무에 따른 분석 변인들의 통계적 유의차를 검증하기 위해 SPSS 27.0 프로그램을 이용하여 paired t-test을 실시하였다. 이때 유의성 수준은 .05로 설정하였다.
1. 등속성 근기능 검사
발목관절 저측굴곡 동작에 대한 최대근력에서는 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 증가한 것으로 나타났다(t=-3.339, p=.009). 근지구력에서는 두 조건 간 통계적으로 유의한 차이가 나타나지 않았지만, WF 조건이 WOF 조건에 비해 상대적으로 증가한 것으로 나타났다. 발목관절 배측굴곡 동작에 대한 최대근력과 근지구력에서는 두 조건 간 통계적 유의차가 나타나지 않았다(Table 1).
|
|
|
WF |
WOF |
|
Plantar |
Strength |
82.9±7.3* |
74.5±9.0* |
|
Endurance |
538.4±45.8 |
521.1±52.3 |
|
|
Dorsiflexion |
Strength |
24.1±2.2 |
24.2±4.7 |
|
Endurance |
130.8±31.2 |
129.9±33.5 |
|
|
Note. *Significant
difference between WF and WOF |
|||
2. 보행 능력 검사
보행 능력 검사는 OPTOgait 보행분석기를 통해 보행 변인 중 보폭 소요시간(step time), 보폭(step length), 보행속도(speed), 분당 보폭 수(cadence), 한발 지지구간(single support) 비율, 양발 지지구간(double support) 비율을 분석하였다.
보행 동작 시 보폭 소요시간, 보폭, 보행속도, 분당 보폭 수에서는 두 조건 간 통계적으로 유의한 차이가 나타나지 않았다. 또한 보행 동작 시 오른발의 한발 지지구간 비율에서는 두 조건 간 통계적으로 유의한 차이가 나타나지 않았지만, 왼발의 한발 지지구간 비율에서는 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 감소한 것으로 나타났다(t=2.377, p=.041). 양발이 동시에 지면에 접촉하고 있는 시기인 양발 지지구간 비율에서는 두 조건 간 통계적으로 유의한 차이가 나타나지 않았다(Table 2).
|
|
|
WF (with FES) |
WOF (without FES) |
|
Step time (sec) |
Left foot |
0.590±0.073 |
0.624±0.128 |
|
Right foot |
0.621±0.975 |
0.617±0.138 |
|
|
Step length (cm) |
Left foot |
64.7±10.0 |
63.5±7.0 |
|
Right foot |
61.7±8.5 |
61.6±7.8 |
|
|
Speed (m/s) |
1.1±0.3 |
1.0±0.2 |
|
|
Cadence (step/min) |
101.7±16.0 |
103.4±14.6 |
|
|
Single support ratio (%) |
Left foot |
36.7±2.1* |
38.4±2.3* |
|
Right foot |
36.9±1.6 |
36.8±1.5 |
|
|
Double support ratio (%) |
27.6±5.1 |
25.1±1.8 |
|
|
Note. *Significant difference between WF and WOF |
|||
본 연구에서는 FES 적용이 노인의 발목관절 근기능과 보행 능력에 미치는 영향을 분석하기 위해 FES 적용 유무에 따른 WF 조건과 WOF 조건 적용 후 발목관절에 대한 등속성 근기능 검사와 보행 능력 검사를 실시하였다.
노화로 인한 하지 근력 약화와 근육량 감소는 전반적인 신체적 기능 저하 및 신체활동 부족으로 이어지며, 나아가 하지 근골격계 질환을 유발시키는 근원적인 요인으로 작용될 수 있다는 점에서 문제의 심각성이 제기되고 있다(Frisoli, Chaves, Ingham & Fried, 2011). Byun, Lee & Hwang (2016)의 연구에서 노인들은 노화에 따른 하지 근력 감소로 인해 신체활동의 시간이 줄어들게 되며, 이러한 현상은 일상생활에서의 삶의 질에 큰 영향을 미친다고 보고하였다. Park (2016)은 노화로 인한 하지 근력 약화와 같이 노인들에게서 주로 나타나는 신체 기능적 특성 변화는 심각한 사회적 문제로 인식되어져야 하며, 노인들의 지속적인 운동 참여를 통해 하지 근력 강화에 관심을 기울여야 한다고 보고하였다.
본 연구의 결과, 발목관절 저측굴곡근의 최대근력은 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 증가한 것으로 나타났으며, 통계적으로 유의한 차이는 나타나지 않았지만 근지구력에서도 WF 조건이 WOF 조건에 비해 증가한 것으로 나타났다. Park (2015)은 FES 처치 하지 근력 운동 집단과 하지 근력 운동 집단을 비교한 연구에서 실험군이 대조군에 비해 근력 및 근지구력이 유의하게 증가하였으며, 근기능 향상 효과도 상대적으로 높은 것으로 나타났다. 이러한 선행연구의 결과와 같이 본 연구에서도 발목관절 저측굴곡근에 FES를 적용할 경우 노인들의 최대근력 및 근지구력을 비롯한 근육 기능이 향상되는 것으로 나타났다. 특히 FES 적용 시 발목관절 저측굴곡근의 최대근력이 유의하게 증가한 것으로 보아 FES 치료가 저측굴곡근의 근력이 저하된 노인들의 근육 활성 및 발목관절의 기능적 움직임에 긍정적인 효과가 있는 것으로 판단된다. 또한 노인들의 하지 근력 수준이 낙상 발생과 밀접한 관련이 있다고 보고한 Barry & Carson (2004)의 연구 결과와 같이 본 연구에서의 FES 치료를 통한 근력 향상이 노인들의 낙상 예방에 도움을 줄 수 있을 것으로 판단된다.
보행 동작은 일상생활에서 가장 중요한 동작 중 하나이며, 비정상적 보행에서 발생될 수 있는 운동역학적 특성 변화는 노화에 따른 신체적 변화를 예측하기 위한 변수로 활용된다. 노인들의 근기능 저하에 따른 정상적 보행 기능의 상실은 근골격계 질환 및 상해 발생의 위험성을 증가시키는 주요 원인이 된다(Jeong & Choi, 2008). Rose (2003)는 노화가 진행됨에 따라 보행 주기의 증가, 양발 지지구간의 증가, 보폭의 감소, 보행속도의 감소, 분당 보폭 수의 감소 등 보행 기능이 저하되는 특성을 보인다고 하였다. Eom (2006)은 노인들의 보행 능력 저하는 하지 근력 및 운동 기능의 약화와 관련성이 있으며, 이로 인해 지속적인 신체활동 감소를 유발시킨다고 보고하였다.
본 연구에서 보행 동작 시 한발 지지구간 비율은 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 감소한 것으로 나타났다. 또한 보행 동작 시 보폭과 보행속도에서는 두 조건 간 통계적 유의차가 나타나지 않았지만, WF 조건에서 WOF 조건에 비해 보폭과 보행속도가 증가한 것으로 나타났다. 이러한 결과는 보행 능력을 향상시키기 위해서는 하지 근육 중 비복근의 강화가 중요하다고 보고한 Van Abbema et al. (2015)의 연구와 같이 FES 치료가 노인들의 저측굴곡근 기능 향상에 긍정적인 영향을 미친 것으로 판단되며, 이를 통해 보행 동작 시 한발 지지구간 비율 감소, 보폭 및 보행속도 증가와 같이 보행 기능이 향상된 결과를 보인 것으로 판단된다. 보행속도는 보행 능력을 판단하는 주요 지표로써, 보행속도의 증가는 일반적으로 보행 능력이 향상된 것으로 해석된다(Skinner & Effeney, 1985). 본 연구의 결과와 유사하게 Jeong & Choi (2008)의 연구에서도 하지 근력 증가 및 근기능 향상이 보행 동작 시 보폭, 보행속도, 분당 보폭 수를 증가시킨다고 보고하였다. 또한 Beavers et al. (2013)과 Callisaya et al. (2011)은 한발 지지구간 비율은 보행 주기에서 한발이 지면에 접촉하고 있는 시간의 비율을 의미하며, 보행속도 증가 시 지면 접촉 시간이 감소하는 경향을 보인다고 보고하였다. Lee (2005)의 연구에서는 발목관절 스트레칭, 탄성밴드를 이용한 점진적 저항운동, 밸런스 보드를 이용한 평형성 운동으로 구성된 발목관절 근기능 증진 프로그램 적용이 노인들의 보행 및 균형 능력을 향상시키고 낙상을 예방한다고 보고하였다. 따라서 하지 근력과 운동 기능이 약화된 노인들에게 있어서 FES 적용이 보행 기능 향상에 긍정적인 효과를 발생시킬 수 있는 것으로 판단된다.
본 연구에서는 FES 적용이 노인의 발목관절 근기능과 보행 능력에 미치는 영향을 분석하기 위해 모든 피험자를 대상으로 FES 적용 유무에 따른 FES 적용(WF)과 FES 미적용(WOF)의 2가지 조건 적용 후 발목관절에 대한 등속성 근기능 검사와 보행 능력 검사를 실시하였으며, 각각의 측정 결과를 산출하여 분석하였다. 본 연구의 결과, 발목관절 저측굴곡근의 최대근력은 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 증가하였으며, 보행 동작 시 한발 지지구간 비율은 WF 조건이 WOF 조건에 비해 통계적으로 유의하게 감소하였다. 이러한 결과로 볼 때, FES를 활용한 적절한 치료가 하지 근력 및 운동 기능이 약화된 노인들의 근육 활성 및 발목관절의 기능적 움직임에 도움을 줄 수 있을 것으로 판단되며, 보행 기능 향상에도 긍정적인 효과를 발생시킬 수 있는 것으로 판단된다. 하지만 본 연구는 65세 이상 남성만을 대상으로 정적인 상황에서 일회성의 FES 치료를 적용하여 수행되었기 때문에, 본 연구의 결과를 일반화하기 위해서는 다양한 연령 및 성별을 대상으로 동적인 상황에서의 FES 치료 효과 검증 및 FES 치료에 대한 종단적 연구와 같은 후속 연구가 필요할 것으로 판단된다.
References
1. Aggio, D. A., Sartini, C., Papacosta, O., Lennon, L. T., Ash, S., Whincup, P. H., Wannamethee, S. G. & Jefferis, B. J. (2016). Cross-sectional associations of objectively measured physical activity and sedentary time with sarcopenia and sarcopenic obesity in older men. Preventive Medicine, 91, 264-272.
Google Scholar
2. Almeida, G. L., Carvalho, R. L. & Talis, V. L. (2006). Postural strategy to keep balance on the seesaw. Gait & Posture, 23(1), 17-21.
Google Scholar
3. An, C. M. & Won, J. I. (2012). Effects of ankle joint mobilization with movement on lower extremity muscle strength and spatiotemporal gait parameters in chronic hemiplegic patients. Physical Therapy Korea, 19(3), 20-30.
Google Scholar
4. Barry, B. K. & Carson, R. G. (2004). Transfer of resistance training to enhance rapid coordinated force production by older adults. Experimental Brain Research, 159(2), 225-238.
Google Scholar
5. Beavers, K. M., Beavers, D. P., Houston, D. K., Harris, T. B., Hue, T. F., Koster, A., Newman, A. B., Simonsick, E. M., Studenski, S. A., Nicklas, B. J. & Kritchevsky, S. B. (2013). Associations between body composition and gait-speed decline: results from the Health, Aging, and Body Composition study. The American Journal of Clinical Nutrition, 97(3), 552-560.
Google Scholar
6. Bily, W., Trimmel, L., Mödlin, M., Kaider, A. & Kern, H. (2008). Training program and additional electric muscle stimula- tion for patellofemoral pain syndrome: a pilot study. Archives of Physical Medicine and Rehabilitation, 89(7), 1230-1236.
Google Scholar
7. Byun, J. J., Lee, K. S. & Hwang, B. G. (2016). An analysis of ankle range of motion, balance and leg muscle strength according to experienced falls in elderly people. Journal of Sport and Leisure Studies, 64(2), 909-916.
8. Callisaya, M. L., Blizzard, L., Schmidt, M. D., Martin, K. L., McGinley, J. L., Sanders, L. M. & Srikanth, V. K. (2011). Gait, gait variability and the risk of multiple incident falls in older people: a population-based study. Age and Ageing, 40(4), 481-487.
Google Scholar
9. Campbell, A. J., Spears, G. F. & Borrie, M. J. (1990). Examination by logistic regression modelling of the variables which increase the relative risk of elderly women falling com- pared to elderly men. Journal of Clinical Epidemiology, 43(12), 1415-1420.
Google Scholar
10. Carr, D. (2021). COVID-19: trends, disparities, and consequences for older adults. The Journals of Gerontology: Series B, 76(3), e65-e67.
Google Scholar
11. Chae, J., Fang, Z. P., Walker, M. & Pourmehdi, S. (2001). Intra- muscular electromyographically controlled neuromuscular electrical stimulation for upper limb recovery in chronic hemiplegia. American Journal of Physical Medicine & Rehabilitation, 80(12), 935-941.
Google Scholar
12. Chekanov, V., Rayel, R., Krum, D., Alwan, I., Hare, J., Bajwa, T. & Akhtare, M. (2002). Electrical stimulation promotes angio- genesis in a rabbit hind-limb ischemia model. Vascular and Endovascular Surgery, 36(5), 357-366.
Google Scholar
13. Cooper, R. L., Taylor, N. F. & Feller, J. A. (2005). A randomised controlled trial of proprioceptive and balance training after surgical reconstruction of the anterior cruciate ligament. Research in Sports Medicine, 13(3), 217-230.
Google Scholar
14. Crameri, R. M., Weston, A., Climstein, M., Davis, G. M. & Sutton, J. R. (2002). Effects of electrical stimulation-induced leg training on skeletal muscle adaptability in spinal cord injury. Scandinavian Journal of Medicine & Science in Sports, 12(5), 316-322.
Google Scholar
15. Cromwell, R. L. & Newton, R. A. (2004). Relationship between balance and gait stability in healthy older adults. Journal of Aging and Physical Activity, 12(1), 90-100.
Google Scholar
16. Eom, J. Y. (2006). A study on the elderly patients hospitalized due to fall injuries. Womens Health, 7(2), 47-68.
17. Frisoli Jr, A., Chaves, P. H., Ingham, S. J. M. & Fried, L. P. (2011). Severe osteopenia and osteoporosis, sarcopenia, and frailty status in community-dwelling older women: results from the Women's Health and Aging Study (WHAS) II. Bone, 48(4), 952-957.
Google Scholar
18. Gaines, J. M., Metter, E. J. & Talbot, L. A. (2004). The effect of neuromuscular electrical stimulation on arthritis knee pain in older adults with osteoarthritis of the knee. Applied Nursing Research, 17(3), 201-206.
Google Scholar
19. Gardner, M. M., Robertson, M. C. & Campbell, A. J. (2000). Exercise in preventing falls and fall related injuries in older people: a review of randomised controlled trials. British Journal of Sports Medicine, 34(1), 7-17.
Google Scholar
20. Gillespie, L. D., Gillespie, W. J., Robertson, M. C., Lamb, S. E., Cumming, R. G. & Rowe, B. H. (2003). Interventions for preventing falls in elderly people. Cochrane Database of Systematic Reviews, 4.
Google Scholar
21. Granat, M. H., Ferguson, A. C. B., Andrews, B. J. & Delargy, M. (1993). The role of functional electrical stimulation in the rehabilitation of patients with incomplete spinal cord injury-observed benefits during gait studies. Spinal Cord, 31(4), 207-215.
Google Scholar
22. Ha, N. R., Kim, M. C. & Han, S. K. (2013). The correlation between changes of ankle joint position sense and sway area through unstable surface training. The Journal of The Korea Institute of Electronic Communication Sciences, 8(9), 1383-1389.
Google Scholar
23. Jeong, S. H. & Choi, D. W. (2008). The effects of 16 weeks' dance sports program on the balance and gait ability in elderly women. The Korean Journal of Growth and Development, 16(3), 225-231.
24. Jeon, M. Y. (2001). Effect of the fall preventon program (FPP) on gait, balance and muscle strength in elderly women at nursing home. Ph.D. Dissertation, Seoul National University.
25. Kaplan, R. E., Czyrny, J. J., Fung, T. S., Unsworth, J. D. & Hirsh, J. (2002). Electrical foot stimulation and implications for the prevention of venous thromboembolic disease. Throm- bosis and Haemostasis, 88(2), 200-204.
Google Scholar
26. Karamanidis, K. & Arampatzis, A. (2011). Altered control strategy between leading and trailing leg increases knee adduction moment in the elderly while descending stairs. Journal of Biomechanics, 44(4), 706-711.
Google Scholar
27. Kim, D. K. (2012). Effect of pre-operative home-based exercise on knee strength and proprioceptive functions after anterior cruciate ligament reconstruction. The Asian Journal of Kinesiology, 14(1), 57-65.
Google Scholar
28. Kirkwood, R. N., Trede, R. G., de Souza Moreira, B., Kirkwood, S. A. & Pereira, L. S. M. (2011). Decreased gastrocnemius temporal muscle activation during gait in elderly women with history of recurrent falls. Gait & Posture, 34(1), 60-64.
Google Scholar
29. Klass, M., Baudry, S. & Duchateau, J. (2011). Modulation of reflex responses in activated ankle dorsiflexors differs in healthy young and elderly subjects. European Journal of Applied Physiology, 111, 1909-1916.
Google Scholar
30. Kontis, V., Bennett, J. E., Mathers, C. D., Li, G., Foreman, K. & Ezzati, M. (2017). Future life expectancy in 35 industrialised countries: projections with a Bayesian model ensemble. The Lancet, 389(10076), 1323-1335.
Google Scholar
31. Lee, S. E. (2005). Effects of increasing ankle range of motion program on ambulation and balance for the elderly with balance disorder. Physical Therapy Korea, 12(2), 28-36.
Google Scholar
32. Lin, Z. & Yan, T. (2011). Long-term effectiveness of neuro- muscular electrical stimulation for promoting motor re- covery of the upper extremity after stroke. Journal of Rehabilitation Medicine, 43(6), 506-510.
Google Scholar
33. Maffiuletti, N. A., Zory, R., Miotti, D., Pellegrino, M. A., Jubeau, M. & Bottinelli, R. (2006). Neuromuscular adaptations to electrostimulation resistance training. American Journal of Physical Medicine & Rehabilitation, 85(2), 167-175.
Google Scholar
34. Mathers, C. D., Stevens, G. A., Boerma, T., White, R. A. & Tobias, M. I. (2015). Causes of international increases in older age life expectancy. The Lancet, 385(9967), 540-548.
Google Scholar
35. Menz, H. B., Morris, M. E. & Lord, S. R. (2006). Foot and ankle risk factors for falls in older people: a prospective study. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 61(8), 866-870.
Google Scholar
36. Miller, C. A. (2002). The connection between drugs and falls in elders. Geriatric Nursing, 2(23), 109-110.
Google Scholar
37. Mir, S. M., Hadian, M. R., Talebian, S. & Nasseri, N. (2008). Functional assessment of knee joint position sense fol- lowing anterior cruciate ligament reconstruction. British Journal of Sports Medicine, 42(4), 300-303.
Google Scholar
38. Park, C. G. (2016). The effect of lower extremity muscles strengthening exercise on health related fitness in elderly women. Journal of Korea Entertainment Industry Associ- ation, 10(6), 165-173.
39. Park, J. L. (2015). The effects of electrical muscle stimulation on the muscular function and balance ability. Ph.D. Dis- sertation, Kyung Hee University.
40. Pekindil, Y., Sarikaya, A., Birtane, M., Pekindil, G. & Salan, A. (2001). 99mTc-sestamibi muscle scintigraphy to assess the response to neuromuscular electrical stimulation of normal quadriceps femoris muscle. Annals of Nuclear Medicine, 15(4), 397-401.
Google Scholar
41. Petersen, N. T., Taylor, J. L. & Gandevia, S. C. (2002). The effect of electrical stimulation of the corticospinal tract on motor units of the human biceps brachii. The Journal of Physiology, 544(1), 277-284.
Google Scholar
42. Romero, J. A., Sanford, T. L., Schroeder, R. V. & Fahey, T. D. (1981). The effects of electrical stimulation of normal quadriceps on strength and girth. Medicine and Science in Sports and Exercise, 14(3), 194-197.
Google Scholar
43. Rose, D. J. (2003). A Comprehensive balance and mobility training program. Human Kinectics.
44. Skinner, H. B. & Effeney, D. J. (1985). Gait analysis in amputees. American Journal of Physical Medicine & Rehabilitation, 64(2), 82-89.
Google Scholar
45. Talbot, L. A., Gaines, J. M., Ling, S. M. & Metter, E. J. (2003). A home-based protocol of electrical muscle stimulation for quadriceps muscle strength in older adults with osteo- arthritis of the knee. The Journal of Rheumatology, 30(7), 1571-1578.
Google Scholar
46. Tinetti, M. E. & Ginter, S. F. (1988). Identifying mobility dys- functions in elderly patients: standard neuromuscular examination or direct assessment?. The Journal of the American Medical Association, 259(8), 1190-1193.
Google Scholar
47. Vanderthommen, M., Depresseux, J. C., Dauchat, L., Degueldre, C., Croisier, J. L. & Crielaard, J. M. (2002). Blood flow variation in human muscle during electrically stimulated exercise bouts. Archives of Physical Medicine and Rehabili- tation, 83(7), 936-941.
Google Scholar
48. Van Abbema, R., De Greef, M., Crajé, C., Krijnen, W., Hobbelen, H. & Van Der Schans, C. (2015). What type, or combi- nation of exercise can improve preferred gait speed in older adults? A meta-analysis. BMC Geriatrics, 15, 1-16.
Google Scholar
49. Vaz, M. A., Baroni, B. M., Geremia, J. M., Lanferdini, F. J., Mayer, A., Arampatzis, A. & Herzog, W. (2013). Neuromuscular electrical stimulation (NMES) reduces structural and func- tional losses of quadriceps muscle and improves health status in patients with knee osteoarthritis. Journal of Orthopaedic Research, 31(4), 511-516.
Google Scholar
