Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Seung-Ki An
Moon-Seok Kwon
Jae-Woo Lee
Young-Tae Lim
https://dx.doi.org/10.5103/KJAB.2024.34.2.53 Epub 2024 May 10
Abstract
Objective: The purpose of this study was to analyze the differences in kinematic factors according to stretching treatment, myofascial release treatment, and static stretching treatment conditions during squat.
Method: Twelve males with resistance training experience participated in this study. Participants performed squats without treatment (Pre-Test), and performed squats after treatment with the myofascial release technique (MRT) and static stretching (SS) on different days (post-test). Squat movements were captured using eight motion capture cameras (sampling rate: 250 Hz), and the peak joint angles of the ankle, knee, hip, and pelvis were calculated for each direction. One-way repeated ANOVA and Bonferroni post hoc analyses using SPSS 27 (IBM Corp. Armonk NY, USA) were used to compare the peak joint angle of the lower extremity joints and pelvis among the normal condition (squat without treatment), MRT condition (squat after MRT treatment) and SS condition (squat after static stretching). The statistical significance level was set at .05.
Results: It was observed that the maximum ankle joint flexion angle during squats was statistically reduced under conditions of myofascial release and static stretching (p<.05), in comparison to the scenario where no stretching was performed. Furthermore, static stretching was found to enhance the maximum hip flexion angle during squat (p<.05), whereas the myofascial release stretching technique resulted in the minimal posterior pelvic tilt angle (p<.05).
Conclusion: Employing myofascial release stretching as a preparatory exercise proved to be more efficacious in maintaining body stability throughout the execution of high-intensity squat movements by effectively managing the posterior tilt of the pelvis, as opposed to foregoing stretching or engaging in static stretching.
Keywords
Squat Static stretching Myofascial release techniques Lower extremity joint
스쿼트는 하체 근력 및 파워 향상을 위한 대표적인 운동으로, 특히 엉덩 관절과 무릎 관절의 가동범위와 안정성이 중요하게 작용한다(Lorenzetti et al., 2018; Myer et al., 2014; Schoenfeld, 2010). 스쿼트 동작은 다관절 운동으로 하지 전체 근육의 활성화를 유발하여 근력을 강화하기 위해 자주 실행되는 운동이다. 특히, 엉덩 관절 주변 근육의 역할이 매우 중요하며(Caterisano et al., 2002), 스쿼트 수행 중 골반의 안정성을 유지하고 중량을 들어올릴 때 필요한 강력한 힘을 생성하는데 중요한 역할을 한다(Caterisano et al., 2002; Clark, Lambert & Hunter, 2012).
엉덩 관절 주변에는 큰볼기근, 중간볼기근, 작은볼기근 등의 폄근과 큰허리근, 엉덩근 등의 굽힘근이 위치하는데, 이들 근육의 적절한 힘과 유연성은 스쿼트 동작 시 골반과 하체의 안정성 유지에 필수적이다(Clark et al., 2012; Mendiguchia, Garrues, Cronin & Contreras, 2020). 특히 큰볼기근과 큰허리근은 스쿼트 시 주요 동력원으로 작용한다(Contreras, Vigotsky, Schoenfeld, Beardsley & Cronin, 2015; Kubo, Oda & Akagi, 2021). 엉덩 관절 굽힘근인 엉덩근과 큰허리근의 단축과 약화는 골반 전방 기울임과 허리 과신전을 유발하여 요부 과부하를 초래할 수 있다(Kendall, McCreary, Provance, Rodgers & Romani, 2005). 반면 엉덩 관절의 바깥돌림근인 궁둥구멍근의 단축은 골반 후방 기울임과 허리 과굽힘을 유발하여 압박 골절 위험을 높인다(Fransen, D'Hooghe, van den Brande, Helsen & Vissers, 2009). 이처럼 엉덩 관절 주변 근육의 불균형은 골반과 허리의 정렬 이상을 초래하여 요부 부상 위험을 높이므로(Nelson & Bandy, 2021), 이 근육군의 적절한 길이와 근력 확보가 중요하다. 엉덩이 근육이 피로하거나 경직되어 있으면, 근육의 길이가 짧아져 스쿼트 동안 근육의 유연성이 감소하고 관절의 가동성이 제한되며, 이는 근육의 수축력을 감소시켜 힘의 효율적인 전달을 방해한다(Marchetti et al., 2017; Van Dillen, Bloom, Gombatto & Susco, 2008). 또한, 이러한 근육의 짧아짐은 스쿼트 동안의 자세 유지 능력을 약화시켜 신체를 불안정한 상태로 만들고 부상 위험을 높일 수 있다(Ekstrom, Donatelli & Carp, 2007; Kasim, 2007). 따라서 통증완화와 관절가동범위의 개선을 위해 스트레칭을 포함한 여러 운동요법들이 수행되고 있으며, 이러한 운동요법들은 관절가동범위를 늘리는 것을 목적으로 권장되고 있다(Braddom, 1996; Shin & Lee, 2006).
스트레칭은 근육을 길게 늘리는 동작을 통해 신체의 움직임을 본격적으로 시작하기 전에 이루어지는 사전 운동이다(Bacurau et al., 2009; Behm & Chaouachi, 2011; Chon & Chang, 2010; Kang & Kim, 2019; Kim & Kim, 2010). 주된 목적은 분야와 응용에 따라 다를 수 있으나, 근육을 늘리고 신체 온도를 상승시켜 전반적인 신체의 준비 상태를 개선하는 데 있다(Behm & Chaouachi, 2011; Samuel, Holcomb, Guadagnoli, Rubley & Wallmann, 2008; Unick, Kieffer, Cheesman & Feeney, 2005). 스트레칭을 통해 상승한 근육 온도는 운동 정보 전도 속도를 증가시키고, 관절의 가동성 및 유연성을 향상시켜 상해 위험을 감소시키는 기대 효과로 인해 많은 스포츠 참가자들에게 권장되고 있다(Chon & Chang, 2010; Lim, Son, Park, Jeng & Kim, 2009; Shrier, 2004; Suh, Hong & Lee, 2006). 그러나 최근 연구들은 운동 전 스트레칭이 실제 운동 수행에 미치는 영향에 대해 재고하고, 운동 목적에 적합한 스트레칭 방식의 적용을 제안하고 있다(Behm & Chaouachi, 2011).
정적 스트레칭은 운동 참여자들 사이에서 오랫동안 선호되어 온 대표적인 사전 운동 방법 중 하나이다. 이 방법은 관절을 일정 기간 동안 굽히거나 폄 시켜 관절의 이동범위를 증가시키고, 근육과 건을 통해 뼈로 힘을 전달하는 MTU (musculotendinous unit)에 영향을 준다(Bandy, Irion & Briggler, 1997; Kim & Shin, 2020; Lee, Yook, Ko, Park & Lee, 2005). 정적 스트레칭은 긴장된 근육을 이완시켜 근육의 혈류를 증가시키며, 이를 통해 신체적 편안함을 제공하고 근력의 비대칭성을 줄이는 데 효과적인 보존적 방법으로 사용된다(Lee et al., 2005; Samuel et al., 2008; Suh et al., 2006). 그러나, 정적 스트레칭에 관한 일부 연구는 이 방식이 근육과 건의 신장성 수축에 대한 내성을 만들어, 순간적인 가속이나 폭발적인 힘을 요구하는 신체 운동 기능을 저하시킬 수 있다고 보고하고 있다(Bacurau et al., 2009; Behm & Chaouachi, 2011; Shrier, 2004).
근막이완기법은 근육과 그 주변 조직인 근막에 집중하여 이를 효과적으로 이완시키는 스트레칭 방법이다(Beardsley & Škarabot, 2015). 이 기법은 근막에 압력을 가하여 통증을 줄이고, 긴장된 근육을 스트레칭 하며, 약한 근육을 강화하고, 관절의 가동범위를 확장하는 것을 목적으로 한다(Kalichman & David, 2017). 근막이완기법은 특히 근육의 탄력성 증가와 연조직의 기능성 복원에 초점을 맞추며, 근막을 직접적으로 자극하여 근육 통증을 줄이고 근육의 길이 변화를 감지하는 신장반사 기능을 개선하는 데 효과적이다(Healey, Hatfield, Blanpied, Dorfman & Riebe, 2014). 이 방법의 적용과 해석은 주로 정적 자세에서 특정 근육에 초점을 맞춘 중재 방법의 결과로 나타난다(Healey et al., 2014; Kim, Kim, Jung & Weon, 2014; Muragod, Patil, Raval & Hiremath, 2018). 그러나 이 기법의 효과는 주로 정적 상황에 대한 연구에서 언급되었으며, 신체 운동의 가속과 근육의 수축과 이완이 유기적으로 수행되는 동적 중량부하 운동에서의 효과에 대해서는 아직 더 많은 탐색이 필요한 상태이다.
따라서, 이 연구는 스쿼트 동작 수행 시 정적 스트레칭과 근막이완기법이 하지 관절의 운동학적 요인에 미치는 영향을 분석하는 것을 목표로 하였다. 본 연구를 통해, 대표적인 부하 운동인 스쿼트를 수행함에 있어서, 부상 위험 감소 및 운동 수행 능력 향상을 위한 근육의 이완과 관절의 유연성 증진에 기여하는 사전 운동 방법의 효과에 대한 정량적 정보를 제시하고자 하였다. 이는 스쿼트와 같은 부하 운동을 안전하고 효율적으로 수행하기 위한 준비 운동 선택에 근거를 마련해 줄 것이다.
1. 연구대상자
본 연구는 근골격계 손상 이력이 최근 12개월 이내에 없으며, 신체적 불균형이 없는 참가자 중에서 스쿼트 동작을 안정적으로 수행할 수 있는 인원을 대상으로 진행되었다. 참가자 선정 기준에 따라, 웨이트 트레이닝 경험이 1년 이상이며 1-RM (1-repetition maximum) 기준으로 스쿼트 100 kg 이상을 수행할 수 있는 성인 남성 12명이 본 연구에 참여하였다. 참여자의 평균 나이는 23.42±1.16 yrs, 평균 신장은 175.63±4.36 cm, 평균 체중은 75.85±4.26 kg 이었다.
2. 연구절차
연구 참가자들은 실험의 목적, 절차, 그리고 주의사항에 대해 상세히 안내 받은 후, 스판덱스(spandex) 소재 의류로 갈아입었다. 이 연구의 목표는 참가자들이 스쿼트 동작을 사전 테스트로 수행한 후, 근막이완기법이나 정적 스트레칭 처치를 적용하고 그 효과를 사후 테스트를 통해 비교 분석하는 것으로, 참가자들이 사전 테스트 전 준비 운동 및 스트레칭 수행을 제한하였다. 또한, 실험에서 사용하는 중량 부하가 낮고 참가자들이 숙련된 웨이트 트레이닝 경험자임을 고려하여, 별도의 준비 운동이나 스트레칭 없이 실험을 진행하였다.
이후, 연구 참가자들의 신체 주요 관절과 분절 부위에 지름이 15 mm인 반사 마커를 Plug-In-Gait 모델(Vicon, USA) 기준으로 부착하였다. 또한 사용할 바벨(barbell)의 양 끝에도 2개의 반사 마커를 추가로 부착하였다. 스쿼트 수행 공간의 전역 좌표계(global reference frame)를 설정하기 위해 Active Wand를 사용하여 캘리브레이션(calibration)을 실시하였고, X 축은 전후 방향(anterior-posterior, AP), Y 축은 좌우 방향(medial-lateral, ML), Z 축은 수직 방향(vertical, VT)으로 설정하였다. 참가자와 바벨에 부착된 반사 마커의 위치 데이터는 8대의 모션 캡처 카메라(MX-T10S, Vicon, USA)를 통해 수집되었으며, 샘플링 비율은 250 Hz였다.
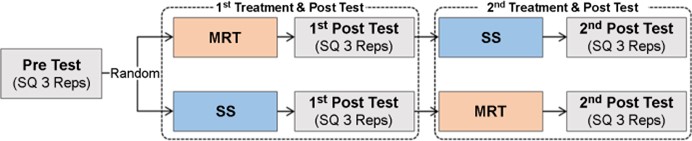
이 연구는 스쿼트 수행 중 근막이완기법과 정적 스트레칭의 효과를 검증하기 위해 설계되었다. 먼저 사전 테스트(pre-test)를 진행한 후, 참가자들에게 근막이완기법(myofascial release technique, MRT) 또는 정적 스트레칭(static stretching, SS) 중 하나를 무작위로 적용하고, 그 이후에 사후 테스트(post-test)를 실시하였다. 연구 참여자는 바벨(barbell)을 양쪽 어깨와 승모근 상부(upper trapezius)에 고정하여 동작을 수행하는 바벨 백 스쿼트(barbell back squat)를 수행했으며, 좌표계 중심 위에 올라가 양 발의 너비는 어깨 너비 정도 벌리고 양 발의 회전 각도는 약 20~30° 외회전 시켜 고정한 뒤, 동작을 실시하였다. 바벨 백 스쿼트 시 스쿼팅 깊이는 최대 깊이로 무릎 굽힘 각도가 120° 깊이로 앉은 동작으로 수행하는 풀 스쿼트(full squat) 방법으로 구분하였다(Lee, Lim & Kwon, 2022). 시작 신호에 맞춰 총 3회 바벨 백 스쿼트를 수행하였다. 이후 무작위로 선정된 근막이완기법 또는 정적 스트레칭을 적용하였고, 사후 테스트는 사전 테스트와 동일한 방식으로 진행되었다. 근막이완기법과 정적 스트레칭의 효과가 중첩될 가능성을 고려하여, 실험은 6명씩 두 조로 나누어 진행되었으며, 첫 번째 조는 근막이완기법 실시 후 1주일 후에 정적 스트레칭을 실시하였고, 두 번째 조는 정적 스트레칭 실시 후 1주일 뒤 근막이완기법을 실시하였다(Figure 1).
1) 근막이완기법(Myofascial Release Technique, MRT)
본 연구에서는 엉덩 관절의 움직임에 기여하는 네 가지 주요 근육인 큰허리근(대요근, Psoas major), 엉덩근(장골근, iliacus), 궁둥구멍근(이상근, Piriformis), 쌍둥이근(쌍자근, gemellus)에 근막이완기법을 적용하였다. 이 근육들은 근경직과 같은 기능적 문제가 발생할 경우 엉덩 관절의 가동성을 제한할 수 있다고 알려져 있다(Gabin, 2009; Neumann, 2002). 근막이완기법의 일관성을 유지하기 위해 숙련된 단 한 명의 처치자가 모든 처치를 담당하였다(Muscolino, 2008). 처치자는 각 근육에 대해 5분씩, 총 20분 동안 처치를 실시했으며(Lee & Nam, 2020), 각 근육에 적용된 구체적인 처치 방법은 <Table 1>에 요약되어 있다.
|
Muscle |
Starting
position |
Method |
Photo |
|
Piriformis |
Side-lying position |
① The subject is
placed on their side with the leg to ② The practitioner
palpates Piriformis and Gemellus, ③ While these muscles are
compressed, the subject ④ The opposite leg is
treated in the same way. |

|
|
Gemellus |
Side-lying position |

|
|
|
Psoas major |
Lying position |
① Prepare the
subject in a lying position. ② The practitioner
palpates the lateral border of the ③ Palpate the exact
location of the Psoas major by |

|
|
Iliacus |
Lying position |
① The subject is
prepared in the supine position. ② The practitioner
places the thumbs of both hands ③ Palpate Iliacus and apply
pressure to them. |

|
2) 정적 스트레칭(Static Stretching)
본 연구에서 실시한 정적 스트레칭(static stretching, SS)은 엉덩 관절의 가동성을 개선하기 위해 선택된 능동적 스트레칭 방법이다. 참가자들은 연구책임자의 지도 아래 총 4가지 스트레칭을 수행하였다. 정적 스트레칭 동안, 참가자들은 각각의 근육군에 통증이 느껴질 직전까지 근육을 신장시킨 후(Lee et al., 2005), 최대 신장 상태를 30초 동안 유지하였다. 이후, 30초 간 휴식을 취하며 이러한 절차를 총 5회 반복하였다. 각 스트레칭 방법의 상세 내용은 <Table 2>에 정리되어 있다.
|
Muscle
group |
Starting position |
Method |
Photo |
|
Hip
joint flexor |
One-leg Kneeling |
① Get into a lunge position with the knee of one leg ②
Move your pelvis forward as far as you can, ③
After 30 seconds, do the same with the other leg. |

|
|
Hip
joint extensor |
Seated position |
① The hip joint of one leg is flexed and abducted, and
the knee joint is bent in a double-legged position ②
The other leg is extended straight behind you. ③
Lean your torso forward as far as possible and ④
After 30 seconds, repeat the same exercise with |

|
|
Hip
joint adductor |
4-point kneeling |
① Lie on your stomach with both knees on the ②
Move your hips backward to relax the hip joint ③
Do this for 30 seconds. |

|
|
Hip
joint posterior |
Lying position |
① Lying on your back, keep one leg straight. The other ②
Use your hands to stabilize the leg with the sole of ③
The hip joint of the leg to be stretched should be ④
After 30 seconds, repeat the exercise on the other leg. |

|
3. 자료처리
Vicon Nexus 2.15 소프트웨어(Vicon, Denver, USA)를 활용해 수집된 데이터에 대한 라벨링과 C3D 파일 형식으로의 추출 작업을 진행하였다. 추출된 각 참가자 별 C3D 파일은 Visual 3D (C-Motion, USA) 소프트웨어를 통해 데이터 처리 및 분석이 이루어졌다. 신체에 부착된 반사 마커의 위치 데이터는 6 Hz의 버터워스 2차 저역통과 필터(butterworth second-order low pass filter)를 사용하여 필터링(filtering) 처리하였다.
스쿼트 수행 시 적용된 처치 방법에 따른 하지 관절 및 골반의 운동학적 변화를 분석하기 위해서, 하지 관절 및 골반의 지역 좌표계(local reference)는 다음과 같이 정의하였다: x 축은 전후 축, y 축은 좌우 축, z 축은 수직 축. 본 연구에 참가한 대상자들은 신체의 불균형이 없는 인원으로 선택되었으며, 백 스쿼트 동작이 양측성 운동인 점을 고려하여 오른쪽 다리를 기준으로 분석 변인을 산출하였다. 이러한 방법으로 산출된 결과는 하지 관절과 골반의 지역 좌표계를 기준으로 정의(Table 3)하였으며, 연구대상자 별 하지 관절 및 골반의 방향 별 각도를 시작 자세를 기준으로 산출하였다. 또한, 전체 구간에서 방향 별 최대 각도를 분석 변인으로 사용하여, 스쿼트 수행 시 적용된 처치 방법의 효과를 평가하였다.
|
Joints & Segment |
Local reference |
||
|
Medial-lateral (ML) axis |
Anterior-posterior (AP) axis |
Superior-inferior (SI) axis |
|
|
Ankle |
+: dorsi flexion |
+: inversion |
+: internal rotation -: external rotation |
|
-: plantar flexion |
-: eversion |
||
|
Knee |
+: extension |
+: adduction |
|
|
-: flexion |
-: abduction |
||
|
Hip |
+: flexion |
+: adduction |
|
|
-: extension |
-: abduction |
||
|
Pelvis |
+: anterior pelvic tilt |
- |
- |
|
-: posterior pelvic tilt |
|||
4. 통계분석
본 연구의 목적은 스쿼트 동작 시 근막이완기법과 정적 스트레칭이 하지 관절의 운동학적 변인에 미치는 영향을 분석하는 것이었다. 이를 위해, 스쿼트 수행 전 아무런 처치를 적용하지 않은 상태를 'Normal' 조건으로, 근막이완기법을 적용한 후 스쿼트를 수행한 상태를 'MRT' 조건으로, 그리고 정적 스트레칭 후 스쿼트를 수행한 상태를 'SS' 조건으로 정의하였다.
백 스쿼트 수행 시 이러한 세 가지 조건(Normal, MRT, SS)에 따른 하지 관절 및 골반의 방향 별 각도 변화를 비교하기 위해, SPSS 27 소프트웨어(Armonk, New York, USA)를 사용하여 일원 반복측정 분산분석(one-way repeated ANOVA)을 실시하였다. 통계적으로 유의미한 결과를 보인 분석 변인들에 대해서는 Bonferroni 사후 분석을 추가로 실시하여, 세 조건 간의 차이를 구체적으로 확인하였다. 통계적 유의수준은 0.05로 설정하였다.
본 연구는 스쿼트 동작 시 근막이완기법(MRT)과 정적 스트레칭(SS)이 하지 관절의 운동학적 변인에 미치는 영향을 분석하는데 초점을 맞추었다. 연구를 위해 세 가지 조건을 설정하였으며, 스쿼트 수행 전 아무런 처치를 적용하지 않은 Normal 조건, 근막이완기법을 적용한 후 스쿼트를 수행하는 MRT 조건, 그리고 정적 스트레칭을 실시한 후 스쿼트를 수행하는 SS 조건을 실시하였다.
이 연구에서는 각 조건 별로 스쿼트 수행 시 하지 관절 및 골반의 운동학적 요인을 비교 분석하였으며 그 결과는 <Table 4>와 같다. 발목 관절의 굽힘/폄 각도에서 Normal 조건에서는 평균 14.15도의 각도를 보여주며 가장 높은 배측 굽힘 각도를 나타냈다. 이는 MRT 조건의 평균 13.74도, SS 조건의 평균 12.68도 보다 높은 수치로, 이 차이는 통계적으로 유의미했다[F=5.737, p=.01]. 그러나 발목 관절의 내번/외번 및 내회전/외회전 각도에서는 세 조건 사이에 통계적으로 유의미한 차이가 나타나지 않았다. 이는 해당 각도 변인들이 이 연구에서 적용한 처치 방법에 의해 크게 영향을 받지 않았음을 의미한다. 무릎 관절에 대한 분석에서는 모든 방향의 최대 각도에서 통계적으로 유의미한 차이가 나타나지 않았다(p>.05). 이는 근막이완기법이나 정적 스트레칭이 무릎 관절의 운동학적 변인에 미치는 영향이 제한적임을 시사한다. 반면, 엉덩 관절의 굽힘/폄 각도에서는 SS 조건이 평균 116.52도로 가장 높은 최대 굽힘 각도를 보였다. Normal 조건의 평균 110.72도와 MRT 조건의 평균 110.06도 보다 높은 수치로, 통계적으로 유의한 차이가 있었다[F=6.370, p=.007]. 사후 분석에서 MRT 조건과 SS 조건[p=.007], 그리고 Normal 조건과 SS 조건[p=.044] 사이에 통계적으로 유의미한 차이가 있었다. 이는 정적 스트레칭이 엉덩 관절의 굽힘/폄 각도에 긍정적인 영향을 미친다는 것을 시사한다. 엉덩 관절의 외전/내전 및 내회전/외회전 각도에서는 세 조건 사이에 유의미한 차이가 없었다[p>.05], 이는 해당 변인들이 스트레칭 방법에 따라 크게 변화하지 않았음을 의미한다. 골반의 최대 전방/후방 기울기 각도에서는 MRT 조건이 평균 -7.8도로 가장 낮은 후방 기울기를 나타내, SS 조건의 평균 -12.33도와 Normal 조건의 평균 -15.64도 보다 낮았다. 이 차이는 통계적으로 유의미했다[F=8.091, p=.002]. 사후 분석 결과, Normal 조건과 MRT 조건 사이에 통계적으로 유의한 차이가 있었다[p=.003]. 이 결과는 근막이완기법이 골반의 후방 기울기를 줄이는 데 효과적임을 보여주며, 스쿼트 수행 시 신체 정렬에 긍정적인 영향을 미칠 수 있음을 시사한다.
|
Variables |
Treatment method |
F |
p |
|||
|
Normal |
MRT |
SS |
||||
|
Ankle joint |
DF(+)/PF(-) |
14.15±3.70 |
13.74±3.53 |
12.68±4.42 |
5.737 |
.010* |
|
IV(+)/EV(-) |
5.12±1.71 |
5.50±1.36 |
7.45±2.43 |
0.407 |
.670 |
|
|
IR(+)/ER(-) |
-11.98±2.87 |
-12.51±7.26 |
-13.13±5.13 |
0.227 |
.799 |
|
|
Knee joint |
Ext(+)/Flex(-) |
-123.98±6.63 |
-118.72±9.49 |
-120.91±6.70 |
3.430 |
.051 |
|
Add(+)/Abd(-) |
9.43±7.22 |
10.80±6.45 |
8.99±5.31 |
0.492 |
.618 |
|
|
IR(+)/ER(-) |
14.03±11.68 |
12.45±3.05 |
21.60±14.56 |
3.191 |
.061 |
|
|
Hip joint |
Flex(+)/Ext(-) |
110.72±12.92c |
110.06±11.56b |
116.52±12.67b,c |
6.370 |
.007* |
|
Add(+)/Abd(-) |
23.63±6.76 |
24.54±5.71 |
25.81±3.35 |
2.120 |
.144 |
|
|
IR(+)/ER(-) |
11.87±10.59 |
9.16±5.29 |
8.38±11.35 |
2.379 |
.116 |
|
|
Pelvis |
AT(+)/PT(-) |
-15.64±8.71a |
-7.80±6.22a |
-12.33±6.09 |
8.091 |
.002* |
|
Note. Abbreviation. MRT = myofascial
release technique, SS = static stretching, DF = dorsi flexion, PF = plantar
flexion, IV = inversion, EV = eversion, Flex = flexion, Ext = extension, Add
= adduction, Abd = abduction, IR = internal rotation, ER = external rotation,
AT = anterior tilt, PT = posterior tilt a,b,c Statistically significant difference at p < .05, a
= Normal vs. MRT, b = MRT vs. SS, c = Normal vs. SS., *p
<.05 |
||||||
본 연구는 스쿼트 동작 시 정적 스트레칭과 근막이완기법이 하지 관절의 운동학적 요인에 미치는 영향을 탐색함으로써, 사전 운동으로서 스트레칭과 근막이완의 실제적인 효과에 대한 이해를 넓히려는 목적을 가졌다. 스쿼트 운동은 근력과 코어 근육 강화에 매우 효과적이지만, 동시에 높은 강도로 인해 신체 관절에 상당한 부하를 줄 수 있어(Kim, Kwon, Park, Jeon & Weon, 2015; Lorenzetti, Ostermann & Zeidler, 2018), 근골격계 상해를 예방하기 위한 적절한 사전 운동의 수행이 권장되어 왔다(Anderson & Madigan, 2014; Bandy et al., 1997; Lee et al., 2005). 이러한 사전 운동 중 정적 스트레칭은 근육의 긴장을 완화하고 근육의 유연성을 증가시켜 근육 손상의 위험을 감소시키는 방법으로 널리 알려져 있다. 정적 스트레칭은 근육이 과도하게 수축되었거나 피로한 상태에서 운동 수행을 할 경우, 상해 위험을 증가시킬 수 있기 때문에(Suh et al., 2006; Sung, 2014), 운동 전후에 스트레칭으로 근육을 길게 늘려 혈류를 증가시키는 것이 중요하다. 또한, 근막이완기법은 근육뿐만 아니라 인접한 조직인 근막을 이완시켜 근육의 유연성을 향상시키고 근육 손상 위험을 줄이는데 기여한다는 점에서 주목받고 있다(Beardsley & Škarabot, 2015; Heo & Park, 2021). 이러한 맥락에서 본 연구는 스트레칭이 실시되지 않은 조건과 근막이완기법, 정적 스트레칭이 적용된 조건에서의 스쿼트 동작 수행 시 하지 관절의 운동학적 변인을 비교 분석하였다. 스쿼트 시 엉덩 관절의 최대 굽힘 각도는 정적 스트레칭을 수행한 경우가 다른 두 조건에 비해 유의하게 높게 나타났다. 이는 정적 스트레칭이 엉덩 관절의 유연성을 증가시키고 더 큰 범위의 운동을 가능하게 함으로써(An & Lee, 2023), 스쿼트 동작 중 엉덩 관절의 운동 범위를 확장하는데 기여할 수 있음을 보여준다. 한편, 근막이완기법은 스쿼트 수행 시 골반의 최대 전후방 기울기 각도에 영향을 미쳤다. 이는 골반과 엉덩 관절의 안정성을 높이고 요추 관절의 상해 위험을 낮출 수 있음을 시사하며, 자가근막이완 운동이 요통환자들에게 엉덩 관절 굽힘, 외회전, 내회전 ROM의 증가와 통증 개선에 미치는 영향을 확인하였던 선행 연구 결과와 유사한 결과를 얻었다(Heo & Park, 2021). 특히 근막이완기법이 스쿼트 수행 전 적용될 경우 골반의 과도한 후방 기울어짐을 억제하는데 효과적일 수 있음을 의미한다.
이러한 결과들은 스트레칭과 근막이완기법이 스쿼트 운동 전 사전 운동으로서 각각의 장점을 가지고 있음을 보여준다. 정적 스트레칭은 엉덩 관절의 가동범위를 확장하는 데 기여할 수 있지만, 발목 관절의 가동성에는 부정적인 영향을 미칠 수 있다. 반면, 근막이완기법은 골반과 엉덩 관절의 안정성을 높이는 데 유용하며, 골반의 후방 기울기를 감소시켜 운동 수행 시 안정성을 증가시킬 수 있다. 이러한 사실은 스쿼트와 같은 운동을 수행하기 전에 개인의 목표와 필요에 따라 가장 적절한 사전 운동 방법을 선택하는 것이 중요함을 강조한다. 따라서, 운동 성능을 최적화하고 부상 위험을 최소화하기 위해서는 스쿼트 수행 전 사전 운동으로 정적 스트레칭과 근막이완기법을 적절히 조합하여 사용하는 것이 바람직할 수 있다. 이와 같은 접근은 개인의 신체 조건, 운동 능력, 그리고 특정 운동의 요구 사항을 고려하여 맞춤화된 프로그램을 설계하는 데 있어서 중요한 기준이 될 것이다.
본 연구는 스쿼트 동작 수행 전 정적 스트레칭과 근막이완기법의 효과를 비교 분석하여, 사전 운동이 하지 관절의 운동학적 요인에 미치는 영향을 평가하였다. 연구 결과는 스트레칭을 수행하지 않은 조건에 비해 근막이완기법과 정적 스트레칭을 적용했을 때 발목 관절의 최대 굽힘 각도가 유의하게 작아짐을 보여줬다. 이는 두 사전 운동 방법이 발목 관절의 유연성에 영향을 미친다는 것을 시사한다. 특히, 정적 스트레칭은 엉덩 관절 굽힘 각도를 증가시켜 엉덩이 관절의 가동범위를 확장하는데 기여하는 반면, 근막이완기법은 골반의 후방 기울기 각도를 감소시킴으로써 골반과 하체의 안정성을 증진시키는 데 효과적임을 나타냈다.
근막이완기법이 골반의 후방 기울기를 줄이는 데 효과적이었다는 결과는 이 기법이 골반과 하체의 안정성에 긍정적인 영향을 미칠 수 있음을 의미한다. 이는 스쿼트와 같은 고강도 운동 수행 시 신체의 올바른 정렬을 유지하고, 운동 효율성을 향상시키며, 부상 위험을 감소시키는 데 중요하다. 스트레칭을 하지 않거나 정적 스트레칭을 수행한 상태보다 근막이완기법을 적용했을 때 더 나은 신체 안정성을 확보할 수 있다는 사실은, 스쿼트 수행 전 적절한 사전 운동 선택이 얼마나 중요한지를 강조한다. 정적 스트레칭이 엉덩 관절 굽힘 각도를 증가시켜 엉덩 관절의 가동범위를 확장하는 데 기여한다는 발견은, 이러한 스트레칭 방법이 엉덩이 주변 근육의 유연성을 개선하고 더 깊은 스쿼트 자세를 가능하게 할 수 있음을 시사한다. 하지만 이러한 유연성 증가가 반드시 운동 수행 능력의 향상으로 이어지는 것은 아니며, 개인의 신체적 특성과 운동 목표에 따라 적절한 사전 운동 방법을 선택하는 것이 중요하다.
본 연구는 남성 성인을 대상으로 한 연구로, 결과의 일반화에는 제한이 있다. 성별, 연령, 신체적 능력의 차이는 운동학적 요인에 미치는 사전 운동의 효과를 다르게 할 수 있으므로, 향후 연구에서는 다양한 대상자를 포함하여 이러한 요인들이 결과에 미치는 영향을 추가로 탐색할 필요가 있다. 또한 추가적인 연구에서는 신체 질량 중심이나 지면 반력과 같은 운동역학적인 데이터를 수집하여 분석하는 것이 필요할 것이다. 이를 통해 스쿼트 동작 수행에 대한 더 깊은 이해를 얻을 수 있고, 운동의 효율성과 부상 예방에 도움이 될 수 있을 것이다.
종합하면, 본 연구는 스쿼트 수행 전 정적 스트레칭과 근막이완기법이 하지 관절의 운동학적 요인에 미치는 구체적인 영향을 평가함으로써, 운동 수행 전 사전 운동의 중요성과 적절한 선택에 대한 인식을 높이는 데 기여한다. 특히 근막이완기법이 골반의 후방 기울기를 줄이는 데 효과적임을 발견함으로써, 이 기법이 스쿼트와 같은 운동에서 신체의 안정성을 향상시키는 데 중요한 역할을 할 수 있음을 시사한다.
References
1. Anderson, D. E. & Madigan, M. L. (2014). Healthy older adults have insufficient hip range of motion and plantar flexor strength to walk like healthy young adults. Journal of Biomechanics, 47(5), 1104-1109.
Google Scholar
2. An, G. J. & Lee, G. H. (2023). Effects of PNF Stretching on Lower Extremity Joint Range of Motion and Muscular Function in Taekwondo Sparring Athletes. The Korean Journal of Growth and Development, 31(3), 173-178.
3. Bacurau, R. F. P., Monteiro, G. A., Ugrinowitsch, C., Tricoli, V., Cabral, L. F. & Aoki, M. S. (2009). Acute effect of a bal- listic and a static stretching exercise bout on flexibility and maximal strength. The Journal of Strength & Conditioning Research, 23(1), 304-308.
Google Scholar
4. Bandy, W. D., Irion, J. M. & Briggler, M. (1997). The effect of time and frequency of static stretching on flexibility of the hamstring muscles. Physical Therapy, 77(10), 1090-1096.
Google Scholar
5. Beardsley, C. & Škarabot, J. (2015). Effects of self-myofascial release: A systematic review. Journal of Bodywork and Movement Therapies, 19(4), 747-758.
Google Scholar
6. Behm, D. G. & Chaouachi, A. (2011). A review of the acute effects of static and dynamic stretching on performance. European Journal of Applied Physiology, 111, 2633-2651.
Google Scholar
7. Braddom, R. L. (1996). Practice Issues in the Hospital-Based Rehabilitation Unit. Physical Medicine and Rehabilitation Clinics of North America, 7(1), 31-41.
Google Scholar
8. Caterisano, A., Moss, R. F., Pellinger, T. K., Woodruff, K., Lewis, V. C., Booth, W. & Khadra, T. (2002). The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. Journal of Strength and Conditioning Research, 16(3), 428-432.
Google Scholar
9. Contreras, B., Vigotsky, A. D., Schoenfeld, B. J., Beardsley, C. & Cronin, J. (2015). A Comparison of Gluteus Maximus, Biceps Femoris, and Vastus Lateralis Electromyographic Activity in the Back Squat and Barbell Hip Thrust Exercises. Journal of Applied Biomechanics, 31(6), 452-458.
Google Scholar
10. Chon, S. C. & Chang, K. Y. (2010). The effects of post-isometric contraction stretching combined with antagonist muscle contraction on muscle strength and flexibility. Korean Society of Sport and Leisure Studies, 40(2), 709-717.
11. Clark, D. R., Lambert, M. I. & Hunter, A. M. (2012). Muscle activation in the loaded free barbell squat: A brief review. Journal of Strength and Conditioning Research, 26(4), 1169-1178.
Google Scholar
12. Ekstrom, R. A., Donatelli, R. A. & Carp, K. C. (2007). Electro- myographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. Journal of Orthopaedic & Sports Physical Therapy, 37(12), 754-762.
Google Scholar
13. Fransen, J., D'Hooghe, P., van den Brande, K., Helsen, W. & Vissers, D. (2009). Positive effects of proprioceptive knee bracing on performance in soccer players. Medicine and Science in Sports and Exercise, 41(4), 736-742.
14. Gabin, M. (2009). An investigation into the effects of manual technique targeted towards psoas major muscle on lum- bar range of motion.
15. Healey, K. C., Hatfield, D. L., Blanpied, P., Dorfman, L. R. & Riebe, D. (2014). The effects of myofascial release with foam rolling on performance. The Journal of Strength & Con- ditioning Research, 28(1), 61-68.
Google Scholar
16. Heo, A. S. & Park, J. Y. (2021). Effect of self-myofascial release training on hip joint ROM and pain improvement in patients with chronic low back pain. Journal of Korean Society for the Study of Physical Education, 26(4), 245-253.
Google Scholar
17. Kalichman, L. & David, C. B. (2017). Effect of self-myofascial release on myofascial pain, muscle flexibility, and strength: A narrative review. Journal of Bodywork and Movement Therapies, 21(2), 446-451.
Google Scholar
18. Kang, T. W. & Kim, B. R. (2019). The effects of stretching and strengthening exercise on the pain, pelvic tilt, functional disability index, and balance ability of patients with chronic lower back pain. The Journal of Korean Physical Therapy, 31(1), 7-12.
Google Scholar
19. Kasim, P. (2007). Optimizing squat technique. Strength and Conditioning Journal, 29(6), 10.
20. Kendall, F. P., McCreary, E. K., Provance, P. G., Rodgers, M. M. & Romani, W. A. (2005). Muscles: Testing and function, with posture and pain. Lippincott Williams & Wilkins.
Google Scholar
21. Kubo, Y., Oda, S. & Akagi, R. (2021). Effects of Squat Depth on Muscle Activity in Vastus Lateralis and Semitendinosus Using Functional Magnetic Resonance Imaging. Journal of Strength and Conditioning Research, 35(2), 433-439.
22. Kim, D., Kim, T., Jung, D. & Weon, J. (2014). Effects of the graston technique and self-myofascial release on the range of motion of a knee joint. Journal of the Korean Society of Physical Medicine, 9(4), 455-463.
Google Scholar
23. Kim, J. & Kim, T. (2010). Immediate effects of stretching on hamstring stiffness. Journal of Korean Physical Therapy, 22(1), 1-7.
Google Scholar
24. Kim, S., Kwon, O., Park, K., Jeon, I. & Weon, J. (2015). Lower extremity strength and the range of motion in relation to squat depth. Journal of Human Kinetics, 45(1), 59-69.
Google Scholar
25. Kim, W. & Shin, D. (2020). Correlations between hip extension range of motion, hip extension asymmetry, and com- pensatory lumbar movement in patients with nonspecific chronic low back pain. Medical Science Monitor: Inter- national Medical Journal of Experimental and Clinical Research, 26, 925080.
Google Scholar
26. Lee, H., Yook, D., Ko, W., Park, Y. & Lee, H. (2005). The effects of static stretching and evjenth-hamberg stretching on range of motion of knee joint. Physical Therapy Korea, 12(2), 37-43.
27. Lee, J., Lim, Y. & Kwon, M. (2022). The effect of foot external rotation on postural stability factors during deep squat. Culture and Convergence, 44(3), 1043-1057.
28. Lee, S. H. & Nam, S. M. (2020). Effects of Active Release Technique on Pain, Oswestry Disability Index and Pelvic Asymmetry in Chronic Low Back Pain Patients. Journal of the Korean Society of Physical Medicine, 15(1), 133-141.
Google Scholar
29. Lim, S., Son, J., Park, D., Jeng, S. & Kim, S. (2009). A com- parative study on the muscle energy technique (MET) and stretching exercise effect of hamstring flexibility improve- ment. Journal of Korean Medicine Rehabilitation, 19(1), 201-211.
Google Scholar
30. Lorenzetti, S., Ostermann, M., Zeidler, F., Zimmer, P., Jentsch, L., List, R., Taylor, W. R. & Schellenberg, F. (2018). How to squat? Effects of various stance widths, foot placement angles and level of experience on knee, hip and trunk motion and loading. BMC Sports Science, Medicine and Rehabilitation, 10, 14.
Google Scholar
31. Lorenzetti, S., Ostermann, M. & Zeidler, F. (2018). The Effect of Squat Depth on Multiarticular Muscle Activation in Collegiate Cross-Country Runners. Journal of Strength and Conditioning Research, 32(6), 1605-1614.
Google Scholar
32. Marchetti, P. H., Fioravante, G. Z., da Silva, J. J., Gomes, W. A., Soares, E. G., Pecoraro, S. L., de Freitas, F. S., Magalhães, R. A., SenagaMiyatake, M. M. & Brown, L. E. (2017). Effects of squat amplitude on pelvic tilt and tibial inclination. MOJ Sports Medicine, 1(1), 6-7.
Google Scholar
33. Mendiguchia, J., Garrues, M. A., Cronin, J. B. & Contreras, B. (2020). Effects of hamstring-emphasized neuromuscular training on strength, sprinting, and jumping performance in football players. Scandinavian Journal of Medicine & Science in Sports, 30(3), 521-531.
Google Scholar
34. Muragod, A., Patil, P., Raval, S. A. & Hiremath, P. (2018). Effect of muscle energy technique and active release technique on hip internal and external rotation range of motion and strength in competitive football players: A randomized clinical trial. Indian Journal of Physiotherapy & Occupa- tional Therapy, 12(4).
Google Scholar
35. Muscolino, J. E. (2008). The muscle and bone palpation manual with trigger points, referral patterns and stretching, Elsevier Health Sciences.
Google Scholar
36. Myer, G. D., Kushner, A. M., Brent, J. L., Schoenfeld, B. J., Hugentobler, J., Lloyd, R. S., Vermeil, A., Chu, D. A., Harbin, J. & McGill, S. M. (2014). The back squat: A proposed assessment of functional deficits and technical factors that limit performance. Strength and Conditioning Journal, 36(6), 4-27.
Google Scholar
37. Nelson, R. T. & Bandy, W. D. (2021). Eccentric training and static stretching improve hamstring flexibility of high school males. Journal of Athletic Training, 36(3), 204-209.
Google Scholar
38. Neumann, D. A. (2002). Kinesiology of the musculoskeletal system. St. Louis: Mosby, 25-40.
Google Scholar
39. Samuel, M. N., Holcomb, W. R., Guadagnoli, M. A., Rubley, M. D. & Wallmann, H. (2008). Acute effects of static and ballistic stretching on measures of strength and power. The Journal of Strength & Conditioning Research, 22(5), 1422-1428.
Google Scholar
40. Schoenfeld, B. J. (2010). Squatting kinematics and kinetics and their application to exercise performance. Journal of Strength and Conditioning Research, 24(12), 3497-3506.
Google Scholar
41. Shrier, I. (2004). Does stretching improve performance?: A systematic and critical review of the literature. Clinical Journal of Sport Medicine, 14(5), 267-273.
Google Scholar
42. Shin, H. S. & Lee, K. S. (2006). Effects of combined resistance exercise on range of motion (ROM), grip strength and pain in middle-aged women with shoulder disorder. The Korea Journal of Sports Science, 15(1), 569-577.
43. Suh, J., Hong, S. & Lee, C. (2006). Effectiveness of stretching exercise in the treatment of the iliotibial band friction syndrome. Journal of Korean Orthopedic Sports Medicine, 5(2), 147-154.
Google Scholar
44. Sung, P. S. (2014). A kinematic analysis for shoulder and pelvis coordination during axial trunk rotation in subjects with and without recurrent low back pain. Gait & Posture, 40(4), 493-498.
Google Scholar
45. Unick, J., Kieffer, H. S., Cheesman, W. & Feeney, A. (2005). The acute effects of static and ballistic stretching on vertical jump performance in trained women. The Journal of Strength & Conditioning Research, 19(1), 206-212.
Google Scholar
46. Van Dillen, L. R., Bloom, N. J., Gombatto, S. P. & Susco, T. M. (2008). Hip rotation range of motion in people with and without low back pain who participate in rotation-related sports. Physical Therapy in Sport, 9(2), 72-81.
Google Scholar
