Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Hyun Sik Chang
Hyung Gyu Jeon
Tae Kyu Kang
Kyeongtak Song
Sae Yong Lee
https://dx.doi.org/10.5103/KJAB.2023.33.2.62 Epub 2023 July 12
Abstract
Objective: Although balance training has been used as an effective ankle injury rehabilitation program to restore neuromuscular deficits in patients with chronic ankle instability, it is not effectively used in terms of motor learning. Attentional focusing can be an effective method for improving ankle kinematics to prevent recurrent ankle injuries. This study aimed to 1) evaluate the effects of attentional focus, including internal and external focus, and 2) determine a more effective focusing method for patients with chronic ankle instability to learn balance tasks.
Method: Twenty-four patients with chronic ankle instability were randomly assigned to three groups (external focus, internal focus, and no feedback) and underwent four weeks of progressive balance training. The three-dimensional ankle kinematics of each patient were measured before and after training as the main outcomes. Ensemble curve analysis, discrete point analysis, and post hoc pairwise comparisons were performed to identify interactions between groups and time.
Results: The results showed that (1) the external focus group was more dorsiflexed and everted than the internal focus group; (2) the external focus group was more dorsiflexed than the no feedback group; and (3) the no feedback group was more dorsiflexed than the internal focus group.
Conclusion: Because dorsiflexion and eversion are ankle motions that oppose the mechanism of lateral ankle sprain, using the external focus method during balance training may be more effective in modifying these motions, thereby reducing the risk of ankle sprain.
Keywords
Ankle kinematics Ankle sprain External focus Motor learning Gait
Ankle sprains are among the most common musculoskeletal injuries, accounting for 7.3% of all sports-related injuries (Roos et al., 2017). Approximately 40% of individuals with a history of ankle sprains experience recurring ankle sprains, which aggravate into a pathological condition called chronic ankle instability (CAI) (Doherty et al., 2016; Hertel & Corbett, 2019). Patients with CAI not only experience persistent local symptoms, including a feeling of the ankle giving way, pain, swelling, and weakness (Hertel & Corbett, 2019; Pope et al., 2011) but also experience decreased health-related quality of life and early onset of post-traumatic ankle osteoarthritis (Simon & Docherty, 2018; Wikstrom et al., 2019).
Because CAI has been linked with several causative factors regarding altered neuromuscular control, including deficits in postural control (Simpson et al., 2019), altered muscle activation in ankles, knees, and gluteus muscles (Delahunt, Monaghan & Caulfield, 2006; Jeon, Lee, Park & Ha, 2021; Lin et al., 2021). Abnormal gait mechanics were described by some researchers (Koldenhoven, Hart, Saliba, Abel & Hertel, 2019; Son, Kim, Seeley & Hopkins, 2019). Foot position before heel-strike may significantly influence the repetitive spells of instability experienced by individuals with CAI (Hertel, 2002; Konradsen & Voigt, 2002; Wright, Neptune, van den Bogert & Nigg, 2000). Individuals with CAI have demonstrated an increased inversion position and velocity from 100 ms before heel strike to 200 ms after heel strike and have been more supinated during the initial stance phase; they have also displayed altered inversion /eversion joint moments from heel strike to mid-stance com- pared to healthy controls (Monaghan, Delahunt & Caulfield, 2006). These altered ankle mechanics are believed to be associated with an impaired dynamic defense against external per- turbations, resulting in an increased likelihood of abnormal ankle movements during ambulatory activities. Furthermore, the ankle is the most important region that is highly involved in several sports and functional activities, including walking and running tasks (Sobhani, Dekker, Postema & Dijkstra, 2013; Wu et al., 2002); therefore, based on the above information, it is important to focus on the abnormal ankle kinematics. Therefore, effective interventions are needed to lower the incidence and improve the quality of life via the restoration of gait pathomechanics, including ankle joint deficits.
Balance training is an effective rehabilitation program for patients with CAI and repeated ankle sprains (Hrysomallis, 2007; McKeon et al., 2008). It could restore neuromuscular deficits by enhancing joint proprioceptors to improve mech anoreceptor function and by stimulating muscle spindles to improve muscle activation (Rozzi, Lephart, Sterner & Kuligowski, 1999). Several studies have demonstrated significant improve- ments in gait parameters and postural control in patients with CAI undergoing progressive balance training, which was designed to challenge their sensorimotor systems (Burcal, Trier & Wikstrom, 2017; McKeon et al., 2008). Although clinicians have used balance training for patients with CAI to recover from their deficiencies, it is not effective in terms of motor learning.
Balance training may be improved by adopting the recent findings in motor learning studies, with respect to the effects of attentional focus (Landers, Hatlevig, Davis, Richards & Rosenlof, 2016). Attentional focus, including internal focus (IF) and ex- ternal focus (EF), refers to the process wherein individuals focus their mental resources to specific movements or activities while performing them. The feedback provided by clinicians during rehabilitation sessions is typically directed at the body movements of the learners, thereby emphasizing IF. In contrast, EF is induced when the attention of a patient is directed toward the effects of body movements (Gokeler et al., 2015; Rotem-Lehrer & Laufer, 2007; Wulf, 2013). Although several studies have been published, information on the effects of attentional focus in orthopedic rehabilitation is limited. In addition, it is challenging for clinicians to treat patients who participate in injury prevention or rehabilitation programs and help them recover from recurrent ankle sprains owing to limited time and funds. Therefore, this study was conducted to 1) evaluate the effects of IF and EF instructions on balance training, and 2) determine the effects of attentional focus on learning a balancing task in patients with CAI. Accordingly, we hypothesized that 1) patients in the EF and IF groups would show greater improvements in ankle kinematics during walking than those with no feedback (NF), and 2) EF will be more effective in preventing ankle sprains than IF.
1. Study design and blinding
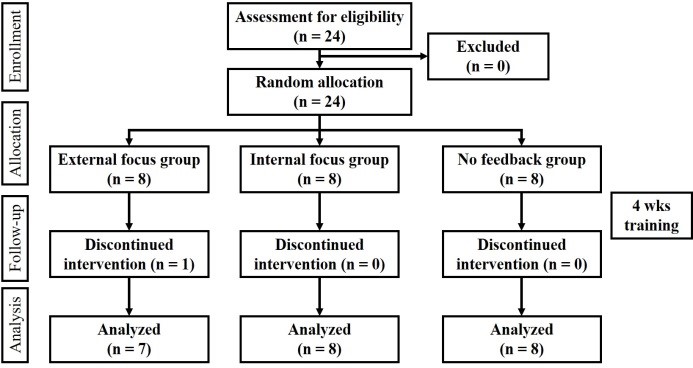
A double-blind randomized controlled trial (RCT) was con- ducted in which neither the data collector nor the subjects were aware of any grouping. The patients with CAI were ran- domly assigned to one of the following three groups: EF, IF, or NF (Figure 1). An independent investigator randomly allocated the patients by opening a sealed envelope containing a se- quential number, which was prepared before study enrollment.
2. Participants
The sample size was determined based on the results of a previous study (McKeon et al., 2008), using G*Power (version 3.164). A priori, repeated-measure analysis of variance (ANOVA) indicated that a sample size of 18 was needed to achieve 80% power for detecting an interaction effect size of .80 (Cohen's d) at a significance level of .05. The variable used for the sample size calculation in the present study was the absolute minimum time-to-boundary, which is one of the main vari- ables examined in studies on patients with CAI. Finally, 24 participants were targeted for the present RCT, with a potential attrition rate of 20%. Twenty-four physically active individuals with self-reported histories of CAI were recruited from intra- mural sports clubs. All participants were involved in moderate or vigorous physical activities, as determined using the Tegner activity scale. The inclusion criteria for CAI were as follows (Gribble et al., 2014): 1) a history of more than one ankle sprain; 2) residual symptoms, including subsequent episodes of the ankle giving way as quantified by a score of <24 on the Cumberland Ankle Instability Tool; and 3) self-reported functional deficits caused by ankle sprains, qualified by a score of <90% on the Foot and Ankle Ability Measure (FAAM) and <80% on the FAAM Sport subscale. The exclusion criteria were as follows: 1) history of lower extremity injury, including ankle sprains, within the past 3 months; 2) history of lower extremity surgery; and 3) balance disorders, neuropathies, diabetes, or other conditions that are known to affect balance. The self-reported worse limbs of the subjects with bilateral CAI were used in this study. This study was approved by the Institutional Review Board of Yonsei University (No. 7001988-202009-BM-294-04), and written informed consent was obtained from all participants prior to their participation.
3. Interventions
Each group completed a 4-week progressive balance train- ing program as described by McKeon et al. (2008) (three sessions of 20 min each per week). This training program was intended to challenge the participants' ability to maintain a single-limb stance during various balance activities, including hopping to stabilization, hopping to stabilization and reach, unanticipated hopping to stabilization, progressive single-limb stance-balancing with open eyes, and progressive single-limb stance-balancing with closed eyes. Over the course of four weeks, the subjects progressed through seven difficulty levels for each activity. The three groups received the same balance training but with different verbal instructions. The EF group was instructed to visually focus on the corn displayed on a meter in front of them during each balance activity. In contrast, the IF group was instructed to concentrate on the foot involved during each balance activity. The NF group was not provided with any additional instructions to perform the balance activity.
4. Procedure and data processing
Before and after four weeks of training, kinematic data during walking were collected using an 8-infrared camera system (MX-F20, Oxford Metric Ltd., Oxford, UK) and a force plate (ORG-6 AMTI, Watertown, Massachusetts, USA) in a laboratory setting. Kinematic data were captured at 200 Hz. Before testing, the anthropometric data of the subjects, including height, weight, limb length, and knee and ankle widths, were obtained to calculate the corresponding internal joint centers. Sixteen reflective markers with double-sided tape were placed on each subject according to a Plug-In-Gait model. The markers were positioned on the anterior superior iliac spine, posterior superior iliac spine, middle portion of the lateral thigh, lateral aspect of the knee joint line, middle position of the lateral shank, lateral malleolus, calcaneal tuberosity, and head of the second metatarsal. To obtain an average walking speed of 1.32 m/s, the subjects were instructed to walk for 2.64 m between 1.905 and 2.105 s. The time required to pass the interval was measured using a running timer (TAKEI TKK 1274; Takei Scientific Instruments, Tokyo, Japan). A sufficient walking practice trial was provided so that the participants could walk as smoothly as possible, and three successful attempts were recorded. All data were collected by an independent investi- gator blinded to the group assignments. The kinematic data from each trial were averaged and resampled to 100 frames, which represented the initial contact to toe-off for the in- volved limb, using a custom program in LabVIEW (version 8.5, National Instruments, Austin, Texas, USA). We analyzed ankle kinematics including 1) peak ankle dorsiflexion, plantar flexion, inversion, and eversion, 2) dorsiflexion and plantar flexion at initial contact, and 3) dorsiflexion and eversion 40 ms before initial contact as independent variables to investigate the group × time interactions and their pairwise comparison.
5. Statistical analysis
Baseline characteristics were compared among groups using one-way ANOVA for continuous variables. To compare the group differences, three separate statistical analyses were per- formed: (1) EF vs. IF, (2) EF vs. NF, and (3) IF vs. NF. Ensemble curve analysis was used to identify the ankle kinematic patterns during walking by calculating the group means and associated 95% confidence intervals (CIs) from initial contact to toe-off, which were then normalized to 100%. Group × time inter- actions on ankle kinematics during walking were determined using two-way repeated-measures ANOVA tests, with the groups as a between-subjects factor and time (pre-test and post-test) as a within-subject factor. Partial eta squared () values were reported as measures of the effect size for ANOVA (≥.01, small; ≥.06, medium; ≥.14, large).
Cohen's d effect sizes and 95% CIs were calculated for post hoc pairwise comparisons to identify the magnitude of the group × time interactions. Data analysis was performed using the Statistical Package for the Social Sciences (SPSS version 23.0; IBM Corp, Armonk, New York, USA).
1. Demographics
No significant group differences were observed in any of the baseline characteristics, including age, height, and weight (Table 1). All 24 subjects were randomly assigned to one of the three balance training groups, and 23 of them completed the training program (Figure 1).
|
|
External |
Internal |
No |
|
(n = 7) |
(n = 8) |
(n = 8) |
|
|
Gender (M:F) |
4:3 |
4:4 |
4:4 |
|
Age (years) |
23.7±1.7 |
22.3±2.8 |
22.6±1.7 |
|
Height (cm) |
177.1±8.0 |
176.0±9.2 |
178.0±10.3 |
|
Weight (kg) |
71.3±12.8 |
70.2±10.4 |
76.1±15.0 |
|
TAS (level) |
6.9±1.9 |
8.0±1.3 |
8.1±1.9 |
|
FAAM (%) |
83.0±9.1 |
80.9±11.2 |
83.1±13.9 |
|
FAAM-Sports (%) |
69.4±8.7 |
65.2±19.9 |
68.3±12.3 |
|
CAIT (score) |
15.1±3.3 |
14.5±5.8 |
13.4±3.5 |
|
Number of ankle |
6.4±3.4 |
9.8±6.8 |
7.3±3.0 |
|
CAIT:
Cumberland Ankle Instability Tool, FAAM: Foot and
Ankle Ability Measure, TAS: Tegner Activity Score |
|||
2. Ensemble curve analysis
1) Difference between external focus and internal focus group
Considering the ankle kinematics of the sagittal plane, the EF group showed greater dorsiflexion (0~95%) during the stance phase in the post-test versus pre-test comparisons (Figure 2A-1). The EF group in the posttest exhibited more dorsiflexion than the IF group in the pretest (0~23%, initial contact to loading response; 90~100%, pre-swing to toe-off) (Figure 2A-2). In addition, the EF group was more dorsiflexed than the IF group in post-test comparisons (0~19%, initial contact to loading response; 53~85%, terminal stance) (Figure 2A-3).
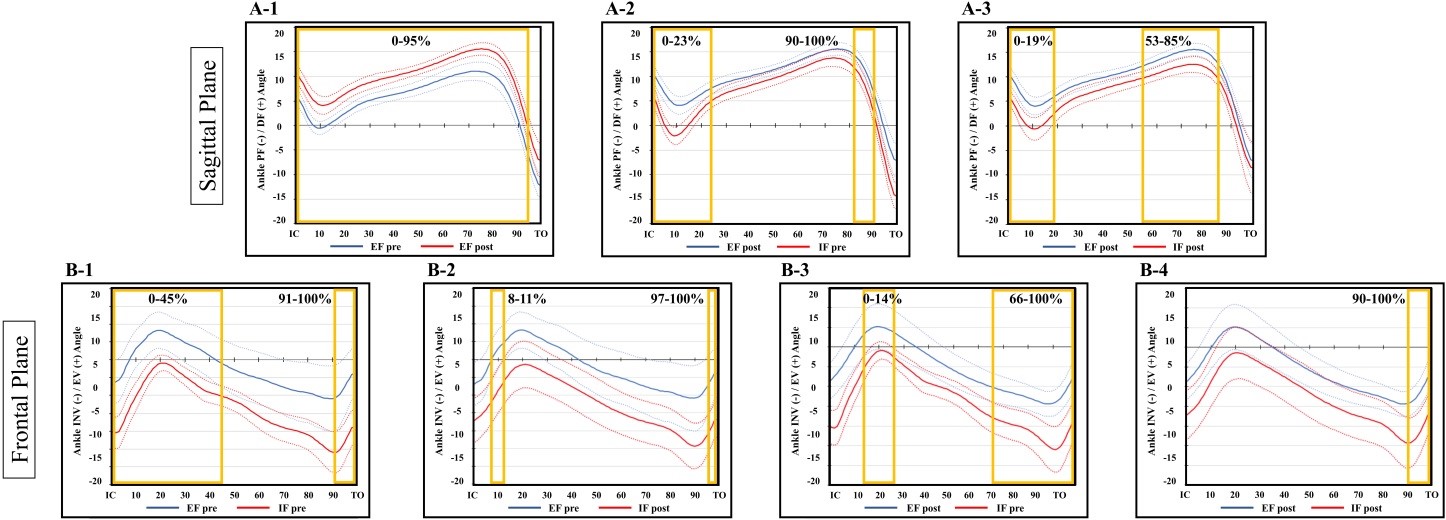
Considering the ankle kinematics of the frontal plane, the IF group was less everted than the EF group in pre-test com- parisons (0~45%, initial contact to mid-stance; 91~100%, pre-swing to toe-off) (Figure 2B-1). In addition, the IF group in the posttest was less everted than the EF group in the pretest (8~11%, loading response; 97~100%, toe-off) (Figure 2B-2). Moreover, the IF group in the pre-test was less everted than the EF group in the post-test (0~14%, initial contact to loading response; 66~100%, terminal stance to toe-off) (Figure 2B-3). Finally, the IF group was more inverted than the EF group in post-test comparisons (90~100%, pre-swing to toe-off) (Figure 2B-4).
2) Difference between external focus and no feed- back group
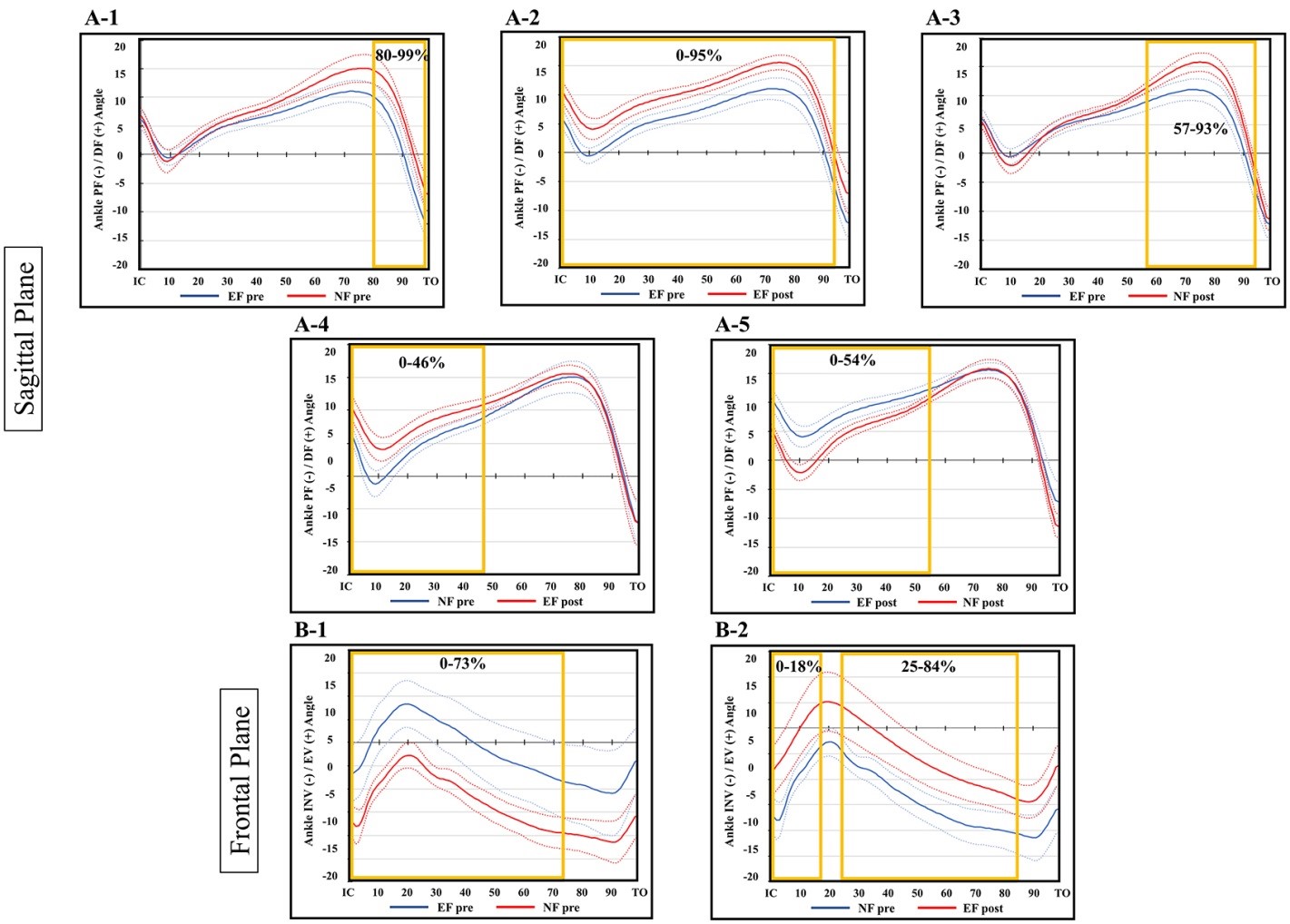
In the sagittal plane, the EF group was less dorsiflexed than the NF group in pre-test comparisons (80~99%, pre-swing to toe-off) (Figure 3A-1). In addition, the EF group showed greater dorsiflexion from 0% to 95% of the stance phase in the posttest to pretest comparisons (Figure 3A-2). Moreover, the EF group in the pre-test was less dorsiflexed than the NF group in the post-test (57~93%, terminal stance to pre-swing) (Figure 3A-3). Furthermore, the EF group in the posttest was more dorsiflexed than the NF group in the pretest (0~46%, initial contact to mid-stance) (Figure 3A-4). Finally, the EF group was more dorsiflexed than the NF group in posttest comparisons (0~54%, initial contact to mid-stance) (Figure 3A-5).
Considering the frontal ankle motion, the NF group was less everted than the EF group in pre-test comparisons (0~73%, initial contact to terminal stance) (Figure 3B-1). Moreover, the NF group in the pre-test was less everted than the EF group in the post-test (0~18%, initial contact to loading response; 25~84%, mid stance to terminal stance) (Figure 3B-2).
3) Difference between internal focus and no feed- back group
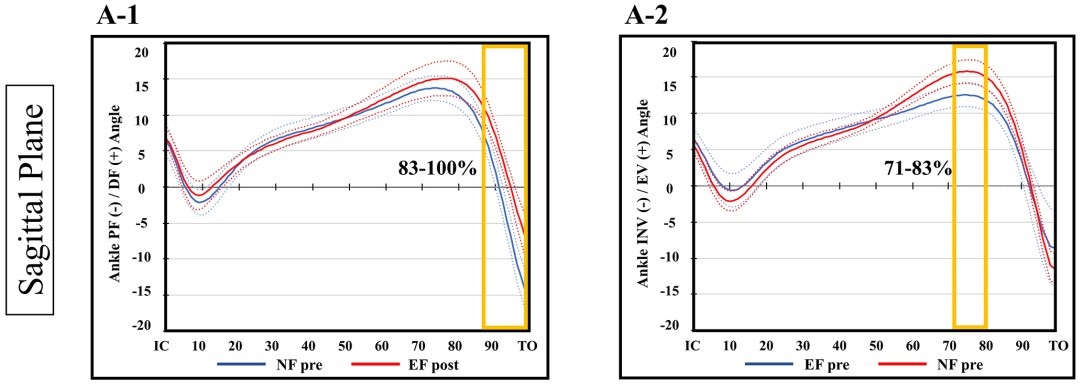
In the sagittal plane, the IF group was less dorsiflexed than the NF group in pretest comparisons (89~100% (pre-swing to toe-off) (Figure 4A-1). In addition, the IF group was less dorsiflexed than the NF group in post-test comparisons (71~ 80%, terminal stance) (Figure 4A-2).
3. Discrete point analysis
1) Difference between external focus and internal focus group
The effect sizes for peak ankle dorsiflexion (F = 3.222, p = .096, = .199), peak ankle eversion (F = .272, p = .611,
= .020), ankle dorsiflexion at initial contact (F = 2.722, p = .123,
= .173), and ankle dorsiflexion 40 ms before initial contact (F = 3.138, p = .100,
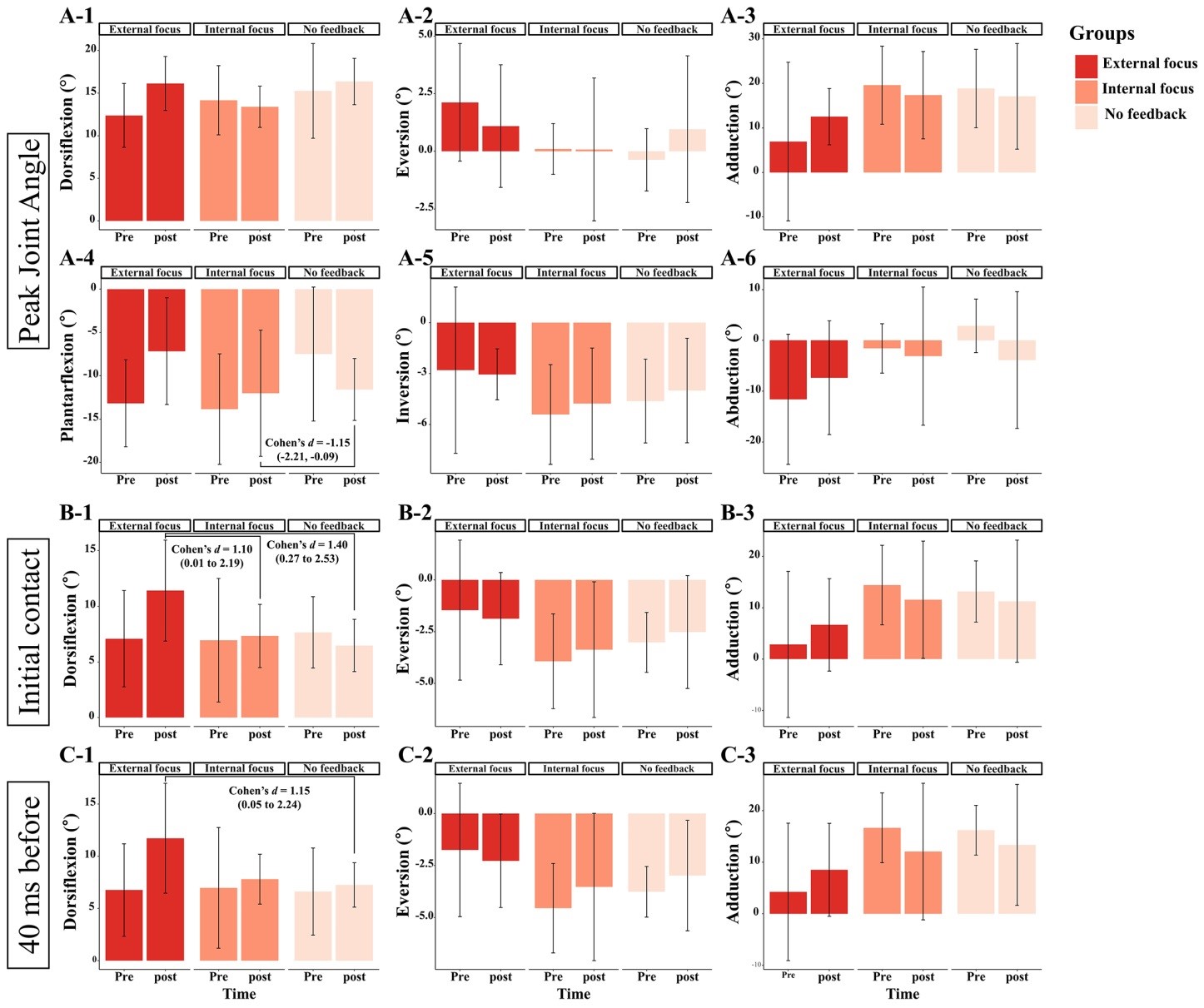
= .194) were sufficiently large to show group × time interactions. The statistically significant pairwise comparison when post-hoc analysis of variables with a large effect size in an ANOVA was as follows: ankle dorsi- flexion at initial contact (post-test of the EF group vs. post-test of the IF group: d = 1.10; 95% CIs = .01 to 2.19) (Figure 5B-1).
The effect size of the group × time interaction in peak ankle plantarflexion was medium (F = .899, p = .360, = .065). The group × time interaction in peak ankle inversion (F = .131, p = .723,
= .010), ankle eversion at initial contact (F = .192, p = .669,
= .015), and ankle eversion at 40 ms before initial contact (F = .463, p = .508,
= .034) exhibited a small effect size. However, none of the time × group interactions with medium or small effect sizes were statistically significant (p < .05).
2) Difference between external focus and no feed- back group
Peak ankle plantar flexion (F = 7.804, p = .015; = .375), ankle dorsiflexion at initial contact (F = 7.800, p = .015;
= .375), and ankle dorsiflexion 40 ms before initial contact (F = 5.838, p = .031;
= .310) showed significant group × time interaction effects with a large effect size. The results of Cohen's d and 95% CIs representing the time × group interactions of significantly different variables were as follows: 1) ankle dorsiflexion at initial contact (post-test of the EF group vs. post-test of the NF group: d = 1.40; 95% CIs = .27 to 2.53) (Figure 5B-1) and 2) ankle dorsiflexion 40 ms before initial contact (post-test of the EF group vs. post-test of the NF group: d = 1.15; 95% CIs = .05 to 2.24) (Figure 5C-1).
The group × time interaction in peak ankle dorsiflexion (F = 1.080, p = .318; = .077) and peak ankle eversion (F = 1.235, p = .287;
= .087) showed a medium effect size. The effect size of group × time interaction in peak ankle inversion (F = .180, p = .679;
= .014), ankle eversion at initial contact (F = .230, p = .639;
= .017), and ankle eversion before 40 ms before initial contact (F = .491, p = .496;
= .036) was small. However, none of the time × group interactions with medium or small effect sizes were statistically significant (p < .05).
3) Difference between internal focus and no feed- back group
No significant group × time interactions were detected; however, the effect size of the peak ankle plantarflexion (F = 2.202, p = .160; = .136) was medium. Furthermore, post-hoc pairwise comparisons showed a significant difference in peak ankle plantarflexion (posttest of the IF group vs. post- test of the NF group: d = -1.15; 95% CIs = -2.21 to -.09) (Figure 5A-4). Except for the peak ankle plantar flexion variable, all other ankle kinematic variables showed small effect sizes (
<.06).
This study was conducted to evaluate the effects of IF and EF instructions and to determine the most effective attentional focus method for balance training in patients with CAI. Our results showed that the EF group was more dorsiflexed and everted than the IF group, the EF group was more dorsiflexed than the NF group, and the NF group was more dorsiflexed than the IF group after aggressive balance training. The effectiveness of attentional focus on ankle kinematics during balance training supports our primary hypothesis.
Changes in ankle kinematics are clinically meaningful, be- cause altered gait mechanics during walking have been reported in individuals with CAI (Delahunt et al., 2006; Drewes et al., 2009; Morrison & Kaminski, 2007). Greater plantarflexion at initial contact and toe-off was observed in patients who experienced ankle sprains than in those with normal ankles (Spaulding, Livingston & Hartsell, 2003). Moreover, researchers have suspected increased supination and combined motions of inversion, plantarflexion, and adduction during the mid-stance phase. It has been suggested that ankle sprains due to inversion occur because of the position of the foot during the stance phase (Hertel, 2002; Morrison & Kaminski, 2007; Tropp, Askling & Gillquist 1985). Moreover, a more plantar flexed and inverted foot position may lead to ankle sprain because the moment arm of the ground reaction force about the subtalar joint increases (Willems, Witvrouw, Delbaere, De Cock & De Clercq, 2005; Wright et al., 2000). Therefore, modifications in the opposite direction of motion to the foot positions that caused by injuries, such as dorsiflexion and eversion, may result in more effective balance training to prevent lateral ankle sprains. The present study supports our hypothesis that applying attentional focus to balance training is more effective than no-feedback intervention in preventing recurrent ankle injuries.
Similar to many other experimental studies comparing the effects of EF and IF using various motor skills (Gokeler et al., 2015; Landers et al., 2016; Laufer, Rotem-Lehrer, Ronen, Khayutin & Rozenberg, 2007; Rotem-Lehrer & Laufer, 2007; Wu, Porter & Brown 2012; Wulf, 2013; Wulf, Zachry, Granados & Dufek, 2007), these studies showed that the EF group was superior to the IF group in terms of motor learning and im- proving physical performance. More specifically, several studies (Landers et al., 2016; McNevin & Wulf, 2002) have shown that EF improves postural stability compared to IF by performing balance tasks. Researchers have reported findings on the same aspects of adopting attentional focus for rehabilitation. Gokeler et al. (2015) demonstrated that EF safely enhances movement patterns to reduce the risk of a second anterior cruciate ligament injury (i.e., knee flexion angle at initial contact, time to peak and peak angles of knee flexion, and range of motion during flexion). Laufer et al. (2007) reported the benefits of adopting EF into three sessions of balance training in patients with acute ankle sprains. Therefore, this study, similar to pre- vious studies, incorporated an additional step in applying the concept of motor learning in clinical trials by utilizing the EF method in rehabilitation programs and demonstrating im- provement in ankle kinematics in individuals with CAI.
In terms of improvements in the ankle kinematics during walking, the EF group was superior to the NF group, and the NF group was superior to the IF group. Our secondary hypothesis that EF is more effective than IF in preventing ankle sprains was supported by these results. The constrained action hypothesis (McNevin, Shea & Wulf, 2003; Wulf, McNevin & Shea, 2001a; Wulf, Shea & Park, 2001b) explains why EF is superior to IF at improving movement performance and quality. IF disrupts automatic motor control processes and regulates coordinated movements to consciously control the motion of the body. In contrast, EF enables unconscious, fast, and reflexive movements to achieve the desired outcome. The outcomes of IF and NF vary because of the difficulty in limiting focus and the human nature of consciously controlling body movements (Wulf, 2013).
However, the IF method may be more beneficial when applied before EF in patients with CAI. Because proprioceptive information from the lateral part of the ankle joint is primarily obtained from the mechanoreceptor of the lateral ligament, and ligament tension is reduced owing to repeated lateral ankle sprains, the degree of inversion angle may be misinter- preted (Konradsen & Voigt, 2002). In other words, patients with CAI exhibited decreased kinesthesia and joint position sense. Balance training is an effective intervention for patients with CAI to enhance kinesthesia and joint position sense, and focusing on ankle joint movement variation via the IF method may maximize the effects of balance training. IF may con- tribute to the recognition or re-education of the sense of joint-position in patients with CAI. By applying EF after recovering balance damaged by trauma, patients and clinicians can expect a gradual increase in difficulty and subsequent improvement because focusing on the movement of one's segment or joint reduces task difficulty.
Clinically, the reason why focusing internally or externally is important for the effective rehabilitation and/or training of patients with CAI is their increased use of visual information (Song, Burcal, Hertel & Wikstrom, 2016). Patients with CAI exhibit decreased somatosensory information from the foot and ankle complexes. Hence, simple verbal cuing may be trivial for training clinicians; however, the impact of atten- tional focusing by simple cues on patients with CAI is further amplified. Furthermore, most studies on attentional focus have measured only certain outcomes, such as conducting motor skills and using attentional focus. In addition, they only used retention tests, which were administered as interventions using attentional focus, to evaluate the same motor skills. However, in the present study, attentional focus was provided only during the balance training. Walking, a different intervention, was used as an outcome measure without attentional focus. Because the intervention and outcome measures were different, this study makes a unique contribution to the field of rehabilitation.
Although we aggressively conducted a balance training program with seven difficulty levels for 4 weeks, there is a possibility that the duration of this training was insufficient to improve muscle control, balance, and function, which could affect the gait patterns of patients with CAI. Most studies on CAI rehabilitation have involved an 8-week training period. Further studies should confirm whether balance training using the attentional focus method can improve the deficits in patients with CAI with respect to various aspects and move- ment patterns compared to traditional training programs that involve a long duration. Moreover, we improved the altered ankle kinematics in the gait pattern, but could not confirm whether it affected subjective ankle instability and the occur- rence of lateral ankle sprain in patients with CAI. It is necessary to confirm whether balance training using attentional focus improves the daily lives of patients with CAI, and whether the training effect can be sustained.
Ankle kinematic differences depended on the type of atten- tional focus after four weeks of balance training. This study showed that the EF group was more dorsiflexed and everted than the IF group, the EF group was more dorsiflexed than the NF group, and the NF group was more dorsiflexed than the IF group. Dorsiflexion and eversion are ankle motions that oppose the mechanism of a lateral ankle sprain, and modifications to these motions may contribute to a reduced risk of ankle sprain. EF was the most effective method, and NF was more effective than IF. To the best of our knowledge, this is the first study to investigate the effects of attentional focus on ankle kinematics during balance training in patients with CAI. Future investigation may involve patients performing more dynamic tasks, such as jogging and landing.
References
1. Burcal, C. J., Trier, A. Y. & Wikstrom, E. A. (2017). Balance training versus balance training with stars in patients with chronic ankle instability: A randomized controlled trial. Journal of Sport Rehabilitation, 26(5), 347-357.
Google Scholar
2. Delahunt, E., Monaghan, K. & Caulfield, B. (2006). Changes in lower limb kinematics, kinetics, and muscle activity in subjects with functional instability of the ankle joint during a single leg drop jump. Journal of Orthopaedic Research, 24(10), 1991-2000.
Google Scholar
3. Doherty, C., Bleakley, C., Hertel, J., Caulfield, B., Ryan, J. & Delahunt, E. (2016). Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: A prospective cohort analysis. American Journal of Sports Medicine, 44(4), 995-1003.
Google Scholar
4. Drewes, L. K., McKeon, P. O., Paolini, G., Riley, P., Kerrigan, D. C., Ingersoll, C. D. & Hertel, J. (2009). Altered ankle kinematics and shank-rear-foot coupling in those with chronic ankle instability. Journal of Sport Rehabilitation, 18(3), 375-388.
Google Scholar
5. Gokeler, A., Benjaminse, A., Welling, W., Alferink, M., Eppinga, P. & Otten, B. (2015). The effects of attentional focus on jump performance and knee joint kinematics in patients after ACL reconstruction. Physical Therapy in Sport, 16(2), 114-120.
Google Scholar
6. Gribble, P. A., Delahunt, E., Bleakley, C., Caulfield, B., Docherty, C. L., Fourchet, F., Fong, D., Hertel, J., Hiller, C., Kaminski, T. W., McKeon, P. O., Refshauge, K. M., van der Wees, P., Vicenzino, B. & Wikstrom, E. A. (2014). Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. Journal of Athletic Training, 49(1), 121-127.
Google Scholar
7. Hertel, J. (2002). Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. Journal of Athletic Training, 37(4), 364-375.
Google Scholar
8. Hertel, J. & Corbett, R. O. (2019). An updated model of chronic ankle instability. Journal of Athletic Training, 54(6), 572-588.
Google Scholar
9. Hrysomallis, C. (2007). Relationship between balance ability, training and sports injury risk. Sports Medicine, 37(6), 547-556.
Google Scholar
10. Jeon, H. G., Lee, S. Y., Park, S. E. & Ha, S. (2021). Ankle in- stability patients exhibit altered muscle activation of lower extremity and ground reaction force during landing: A systematic review and meta-analysis. Journal of Sports Science and Medicine, 20(2), 373-390.
Google Scholar
11. Koldenhoven, R. M., Hart, J., Saliba, S., Abel, M. F. & Hertel, J. (2019). Gait kinematics & kinetics at three walking speeds in individuals with chronic ankle instability and ankle sprain copers. Gait & Posture, 74, 169-175.
Google Scholar
12. Konradsen, L. & Voigt, M. (2002). Inversion injury biomechanics in functional ankle instability: A cadaver study of simulated gait. Scandinavian Journal of Medicine & Science in Sports, 12(6), 329-336.
Google Scholar
13. Landers, M. R., Hatlevig, R. M., Davis, A. D., Richards, A. R. & Rosenlof, L. E. (2016). Does attentional focus during bal- ance training in people with Parkinson's disease affect outcome? A randomised controlled clinical trial. Clinical Rehabilitation, 30(1), 53-63.
Google Scholar
14. Laufer, Y., Rotem-Lehrer, N., Ronen, Z., Khayutin, G. & Rozenberg, I. (2007). Effect of attention focus on acquisition and re- tention of postural control following ankle sprain. Archives of Physical Medicine and Rehabilitation, 88(1), 105-108.
Google Scholar
15. Lin, C. I., Khajooei, M., Engel, T., Nair, A., Heikkila, M., Kaplick, H. & Mayer, F. (2021). The effect of chronic ankle instability on muscle activations in lower extremities. PLOS ONE, 16(2), e0247581.
Google Scholar
16. McKeon, P. O., Ingersoll, C. D., Kerrigan, D. C., Saliba, E., Bennett, B. C. & Hertel, J. (2008). Balance training improves function and postural control in those with chronic ankle instability. Medicine and Science in Sports and Exercise, 40(10), 1810-1819.
Google Scholar
17. McNevin, N. H., Shea, C. H. & Wulf, G. (2003). Increasing the distance of an external focus of attention enhances learn- ing. The International Journal of Psychological Research, 67(1), 22-29.
Google Scholar
18. McNevin, N. H. & Wulf, G. (2002). Attentional focus on supra-postural tasks affects postural control. Human Movement Science, 21(2), 187-202.
Google Scholar
19. Monaghan, K., Delahunt, E. & Caulfield, B. (2006). Ankle func- tion during gait in patients with chronic ankle instability compared to controls. Clinical Biomechanics (Bristol, Avon), 21(2), 168-174.
Google Scholar
20. Morrison, K. E. & Kaminski, T. W. (2007). Foot characteristics in association with inversion ankle injury. Journal of Athletic Training, 42(1), 135.
Google Scholar
21. Pope, M., Chinn, L., Mullineaux, D., McKeon, P. O., Drewes, L. & Hertel, J. (2011). Spatial postural control alterations with chronic ankle instability. Gait & Posture, 34(2), 154-158.
Google Scholar
22. Roos, K. G., Kerr, Z. Y., Mauntel, T. C., Djoko, A., Dompier, T. P. & Wikstrom, E. A. (2017). The epidemiology of lateral ligament complex ankle sprains in national collegiate athletic association sports. The American Journal of Sports Medicine, 45(1), 201-209.
Google Scholar
23. Rotem-Lehrer, N. & Laufer, Y. (2007). Effect of focus of atten- tion on transfer of a postural control task following an ankle sprain. Journal of Orthopaedic & Sports Physical Therapy, 37(9), 564-569.
Google Scholar
24. Rozzi, S. L., Lephart, S. M., Sterner, R. & Kuligowski, L. (1999). Balance training for persons with functionally unstable ankles. Journal of Orthopaedic & Sports Physical Therapy, 29(8), 478-486.
Google Scholar
25. Simon, J. E. & Docherty, C. L. (2018). Health-related quality of life is decreased in middle-aged adults with chronic ankle instability. Journal of Science and Medicine in Sport, 21(12), 1206-1209.
Google Scholar
26. Simpson, J. D., Rendos, N. K., Stewart, E. M., Turner, A. J., Wilson, S. J., Macias, D. M., Chander, H. & Knight, A. C. (2019). Bilateral spatiotemporal postural control impairments are present in participants with chronic ankle instability. Physical Therapy in Sport, 39, 1-7.
Google Scholar
27. Sobhani, S., Dekker, R., Postema, K. & Dijkstra, P. U. (2013). Epidemiology of ankle and foot overuse injuries in sports: A systematic review. Scandinavian Journal of Medicine & Science in Sports, 23(6), 669-686.
Google Scholar
28. Son, S. J., Kim, H., Seeley, M. K. & Hopkins, J. T. (2019). Altered walking neuromechanics in patients with chronic ankle instability. Journal of Athletic Training, 54(6), 684-697.
Google Scholar
29. Song, K., Burcal, C. J., Hertel, J. & Wikstrom, E. A. (2016). Increased visual use in chronic ankle instability: A meta-analysis. Medicine and Science in Sports and Exercise, 48(10), 2046-2056.
Google Scholar
30. Spaulding, S., Livingston, L. & Hartsell, H. (2003). The influence of external orthotic support on the adaptive gait char- acteristics of individuals with chronically unstable ankles. Gait & Posture, 17(2), 152-158.
Google Scholar
31. Tropp, H., Askling, C. & Gillquist, J. (1985). Prevention of ankle sprains. The American Journal of Sports Medicine, 13(4), 259-262.
Google Scholar
32. Wikstrom, E. A., Song, K., Tennant, J. N., Dederer, K. M., Paranjape, C. & Pietrosimone, B. (2019). T1ρ MRI of the talar articular cartilage is increased in those with chronic ankle instability. Osteoarthritis Cartilage, 27(4), 646-649.
Google Scholar
33. Willems, T., Witvrouw, E., Delbaere, K., De Cock, A. & De Clercq, D. (2005). Relationship between gait biomechanics and inversion sprains: a prospective study of risk factors. Gait & Posture, 21(4), 379-387.
Google Scholar
34. Wright, I., Neptune, R., van den Bogert, A. J. & Nigg, B. (2000). The influence of foot positioning on ankle sprains. Journal of Biomechanics, 33(5), 513-519.
Google Scholar
35. Wu, G., Siegler, S., Allard, P., Kirtley, C., Leardini, A., Rosenbaum, D., Whittle, M., D'Lima, D. D., Cristofolini, L., Witte, H., Schmid, O. & Stokes, I., Standardization and Terminology Committee of the International Society of Biomechanics. (2002). ISB recommendation on definitions of joint coord- inate system of various joints for the reporting of human joint motion--part I: Ankle, hip, and spine. International Society of Biomechanics. Journal of Biomechanics, 35(4), 543-548.
36. Wu, W. F., Porter, J. M. & Brown, L. E. (2012). Effect of atten- tional focus strategies on peak force and performance in the standing long jump. Journal of Strength and Con- ditioning Research, 26(5), 1226-1231.
Google Scholar
37. Wulf, G. (2013). Attentional focus and motor learning: A review of 15 years. International Review of Sport and Exercise Psychology, 6(1), 77-104.
Google Scholar
38. Wulf, G., McNevin, N. & Shea, C. H. (2001a). The automaticity of complex motor skill learning as a function of attentional focus. Quarterly Journal of Experimental Psychology, 54(4), 1143-1154.
Google Scholar
39. Wulf, G., Shea, C. & Park, J. H. (2001b). Attention and motor performance: Preferences for and advantages of an ex- ternal focus. Research Quarterly for Exercise and Sport, 72(4), 335-344.
Google Scholar
40. Wulf, G., Zachry, T., Granados, C. & Dufek, J. S. (2007). In- creases in jump-and-reach height through an external focus of attention. International Journal of Sports Science & Coaching, 2(3), 275-284.
Google Scholar
