Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Hee Seong Jeong
Junbom Song
Inje Lee
Doosup Kim
Sae Yong Lee
http://dx.doi.org/10.5103/KJSB.2021.31.3.155 Epub 2021 October 12
Abstract
Objective: There is a lack of studies using the 3D-2D image registration techniques on the mechanism of a shoulder injury for ice hockey players. This study aimed to analyze in vivo 3D glenohumeral joint arthrokinematics in collegiate ice hockey athletes and compare shoulder scaption with or without a hockey stick using the 3D-2D image registration technique.
Method: We recruited 12 male elite ice hockey players (age, 19.88 ± 0.65 years). For arthrokinematic analysis of the common shoulder abduction movements of the injury pathogenesis of ice hockey players, participants abducted their dominant arm along the scapular plane and then grabbed a stick using the same motion under C-arm fluoroscopy with 16 frames per second. Computed tomography (CT) scans of the shoulder complex were obtained with a 0.6-mm slice pitch. Data from the humerus translation distances, scapula upward rotation, anterior-posterior tilt, internal to external rotation angles, and scapulohumeral rhythm (SHR) ratio on glenohumeral (GH) joint kinematics were outputted using a MATLAB customized code.
Results: The humeral translation in the stick hand compared to the bare hand moved more anterior and more superior until the abduction angle reached 40°. When the GH joint in the stick hand was at the maximal abduction of the scapula, the scapula was externally rotated 2~5° relative to 0°. The SHR ratio relative to the abduction along the scapular plane at 40° indicated a statistically significant difference between the two groups (p < 0.05).
Conclusion: With arm loading with the stick, the humeral and scapular kinematics showed a significant correlation in the initial section of the SHR. Although these correlations might be difficult in clinical settings, ice hockey athletes can lead to the movement difference of the scapulohumeral joints with inherent instability.
Keywords
Ice hockey 3D-D registration Scaption Shoulder joint External load
The shoulder complex is a joint that allows for a lot of mobility (Lee, Han & Kang, 2007). Particularly, the glenohumeral (GH) joint, which is a multiaxial ball-and-socket joint, provides a wider range of motion than any other joints in the human body at the cost of decreased stability (Koh, Weon & Jung, 2012). For this reason, various types of injuries occur to the shoulder joint due to its characteristics (Lee, 2009). To prevent injuries and improve performance, sports such as throwing, using a racket, and slapping requires an appropriate range of motion on the GH joint. For example, when a volleyball player hits or con- tacts a ball on the overhead cocking position frequently (Kerr, Collins, Pommering, Fields & Comstock, 2011) or when an ice hockey player performs a slap shot or suffers from a direct blow at the backside, the humerus-scapula motion should be synchronized (Agel & Harvey, 2010; Dwyer, Petrera, Bleakney & Theodoropoulos, 2013; Mölsä, Airaksinen, Näsman & Torstila, 1997; Mölsä, Kujala, Myllynen, Torstila & Airaksinen, 2003).
Especially, ice hockey is a fast and aggressive sport with a high risk of injury. Players can skate at explosive speeds, shoot pucks at a speed of up to 100 miles per hour, and have irregular, frequent body collisions with other players and hockey sticks. The body checking violation and the unintentional collision with an opponent are the common mechanisms of injury (Mölsä, Kujala, Näsman, Lehtipuu & Airaksinen, 2000). For this reason, ice hockey has been categorized to have a high risk for traumatic joint injuries attributed to aggressiveness and random motion characteristics of this contact sport. Besides, the contact points of the sticks held by the players can instantaneously increase the external load applied to the shoulder due to the difference in the moment arm. When ice hockey players hold a stick and make intense movements, the connection length of the arm and stick, that is, in- creasing the length of the moment arm, resulting in increased stress and tension on the shoulder joints and muscles. Tuominen, Stuart, Aubry, Kannus & Parkkari (2015) have investigated the adult and junior world-class competitions initiated by the International Ice Hockey Federation and reported that body checking (27.2%) and stick contact (21.1%) were the most common causes of upper-body injuries (Tuominen et al., 2015; Tuominen et al., 2016). In addition, Mölsä, Kujala, Myllynen, Torstila & Airaksinen (2003) have reported that body checking or collisions between athletes account for 76% of the cause of shoulder injuries, whereas 19% of distal upper extremity injuries are caused by hard blows from sticks.
Mostly, the proportion of shoulder injuries in all joint injuries is the second-highest following knee injuries in ice hockey. Approximately 10% of all injuries occurring in European professional ice hockey players are shoulder injuries (Mölsä et al., 2000). The percentage of shoulder injuries is slightly higher in the United States with 15% for American collegiate ice hockey players and 12% for the National Hockey League (Flik, Lyman & Marx, 2005; McKay, Tufts, Shaffer & Meeuwisse, 2014). Alternatively, in South Korea, shoulder injuries are the most common injuries experienced by ice hockey players, particularly in high school players (Lee, Lee, Lee & Kim, 2014). Therefore, the movement of the humeral head of elite ice hockey athletes in South Korea is worth investigating.
Studies on shoulder motion have used conventional X-ray images (Freedman & Munro, 1966; Inman, Saunders & Abbott, 1996; Poppen & Walker, 1976). However, radiographic studies may not be sufficient for assessing the shoulder complex because shoulder movements are three-dimensional (3D). 3D-two-dimensional (2D) model registration is a 3D assessment technique using fluoroscopic images that were originally developed to measure in vivo 3D kinematics following total knee arthroplasty. Several studies have evaluated the natural knee joint kinematics and anterior cruciate ligament-deficient knee using the 3D-2D model registration technique. However, only a few studies have focused on shoulder kinematics. The 3D-2D model registration tech- nique is a noninvasive and accurate method. Recently, several studies have examined shoulder kinematics using this measurement technique. A study has reported that the accuracy was 0.53 mm for in-plane translation, 1.6 mm for out-plane translation, and 0.54° for rotations (Moro-oka et al., 2007). Thus, this technique provides accurate dynamic kinematic in vivo measurements.
Therefore, this study aimed to analyze in vivo 3D GH joint arthro- kinematics in elite ice hockey players and to compare shoulder scaption with or without a hockey stick using the 3D-2D model registration technique. We hypothesized that: 1) there are statistically significant differences in the GH joint arthrokinematic factors between the shoulder scaption movement with or without a stick. 2) SHR would be a different ratio between the shoulder scaption movement with and without a stick. In the future, we think that the outcomes of this study will be a cornerstone for 3D modeling to prevent injuries, the development of programs to improve performance, and the prevention of shoulder degenerative arthritis in athletes.
1. Participants
We recruited 12 male elite ice hockey players (age, 19.88±0.65 years; height, 178.80±3.00 cm; weight 77.58±6.43 kg). The exclusion criteria included a history of injury in the shoulder joints or an orthopedic history within 3 months. All participants provided informed consent based on the procedures approved by the Institutional Review Board of Human Research.
2. Procedure and data analysis
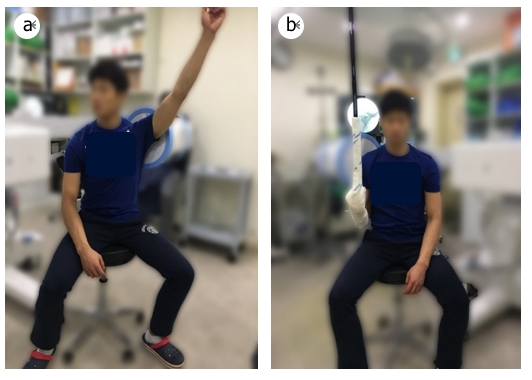
All participants provided written informed consent in compliance with the Institutional Review Board at Yonsei University (IRB No. 7001988-201612-HR-311-02). The participants filled out a questionnaire con- taining questions on a history of injury, disease, or surgery. For arthro- kinematic analysis of the most commonly used shoulder abduction movements of the injury pathogenesis of ice hockey players suitable for the purpose and hypothesis of this study, we measure them in the following positions. The measurement: 1) at the start point zero degrees of shoulder flexion sagittal plane of the dominant's arm, the bare arm raised and raised down 45 degrees of the shoulder horizontal abduction. 2) The arm with stick raised and raised down with 45 degrees of the shoulder horizontal abduction (Figure 1). The length and weight of the hockey sticks used in this study were 165 cm and 535 g, respectively. Each participant conducted arm abduction in the scapular plane to the maximum elevation while keeping the elbow fully extended under C-arm fluoroscopy with 16 frames per second. C-Arm is a mobile imaging unit used for fluoroscopic imaging during surgical and ortho- pedic procedures. It also consists of a computer workstation used to view, manipulate, store and transfer the images. Computed tomography (CT) scans of the shoulder complex were obtained with a 0.6-mm slice pitch. Each motion was performed once per cycle, and two trials were performed. The time required for each action was 5s.
1) Image acquisition and 3D modeling
Each participant abducted their arms along the scapular plane to maximum elevation while keeping the elbow fully extended, under C-arm fluoroscopy (Zen-2090 Pro; Genoray Co., Ltd, Korea) with 16 frames per second. To calibrate barrel distortion of the radiographic projection parameters, we used calibration files by customized CT scans (GE Brightspeed S; GE Healthcare, Milwaukee, WI, USA) of the shoulder complex, which were obtained with a 0.6-mm slice pitch (image matrix, 512×512; pixel size, 0.6×0.6 mm). The CT images were segmented, and 3D models of the humerus and scapula bone were generated (ITK-Snap; Penn Image Computing and Science Laboratory, Philadelphia, PA, USA). Additionally, the bone models were trimmed using the ITK-Snap (Figure 2).

In the study by Matsuki et al. (2011), anatomical coordinate systems were developed in the scapula and humerus models (Geomagic Studio; Raindrop Geomagic, Research Triangle Park, NC, USA). The movement of the humerus to the scapula was defined as abduction along the Z-axis rotation and internal to external rotation along the Y-axis rotation (Figure 2). Anteroposterior (AP) translation of the GH joint was defined as translation relative to the X-axis of the center of the glenoid; supero- inferior (SI) translation was defined as the translation of the humeral head origin relative to the Y-axis of the centroid of the glenoid fossa (Figure 2).
2) Image registration and data processing
The location of the humerus and scapula in the 3D space was matched by a single-plane fluoroscopic image using the 3D-2D model registration technique using a Jointtrack software-based method (www.sourceforge.net/projectsss/jointtrack). Data on GH joint kinematics were outputted using a MATLAB customized code (MathWorks Inc., Natick, MA, USA). The customized code was used to interpolate the humeral abduction angle in 10° increments (In an easy-to-understand way by changing about 10 degrees according to the clinical measure- ment method) and obtain data on the kinematics of the GH joint. The GH kinematic data were described as a motion of the humeral abduction angle, and polynomial regression lines were used to compute interpolating outputs at each 10° increment of arm abduction from rest to maximal abduction position.
3. Statistical analysis
Correlation analysis was performed to compare humerus translation distances, scapula upward rotation, AP tilt, internal to external rotation, and SHR. The independent t-test was performed to statistically analyze whether there are significant differences between the data obtained with or without a stick, between the SI position, AP translation, and internal to external rotation of the humerus, and between the upward rotation of the scapula, AP tilt, internal to external rotation, and SHR. P values of less than 0.05 were used to denote statistical significance.
1. Humeral translation
The humeral AP translation relative to the scapula in shoulder abduc- tion was measured where the humeral head of the stick hand was located approximately 3.5 mm anteriorly, but the bare hand was 1 mm posteriorly in the initial position (Table 1 and Figure 3). No correlation was observed between the bare and stick groups regarding the change of AP-translated position depending on the shoulder abduction angle (R2 = -0.044; p = 0.887).
|
Variables |
Classification |
Bare hand (n = 12) |
Stick hand (n=12) |
p |
|
Humerus A(+) P(-) |
Initial |
-1.14±8.16 |
3.54±7.69 |
0.162 |
|
Maximum |
-0.02±4.4 |
-1.63±7.23 |
0.521 |
|
|
Humerus S(+) I(-) |
Initial |
-0.26±5.6 |
2.36±7.7 |
0.353 |
|
Maximum |
0.33±3.79 |
-2.37±5.04 |
0.150 |
|
|
Scapula upward rotation |
Initial |
2.11±10.24 |
1.38±12.99 |
0.882 |
|
Maximum |
43.35±7.52 |
46.76±9.2 |
0.332 |
|
|
Scapula A(-) P(+)
tilt |
Maximum |
13.52±7.08 |
8.76±8.78 |
0.164 |
|
Scapula IR(-) ER(+) |
Maximum |
2.7±3.95 |
5±6.19 |
0.203 |
|
Scapulohumeral rhythm |
Initial |
1.24±5.38 |
3.24±6.39 |
0.421 |
|
Maximum |
4.17±2.6 |
2.98±1.18 |
0.163 |
|
|
A, anterior; P, posterior;
S, superior; I, inferior; IR, internal rotation; ER, external rotation Values are expressed as
mean ± standard deviation |
||||
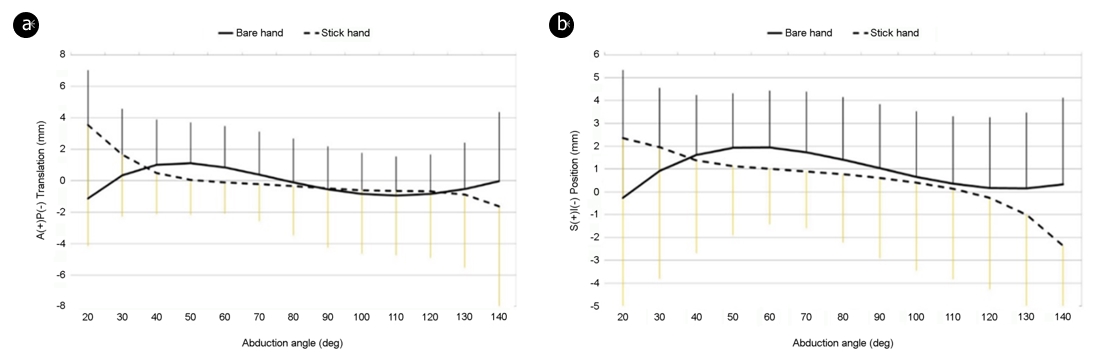
The humeral SI translation relative to the scapula in shoulder abduc- tion was measured where the humeral head of the stick hand was located 2.5 mm more superiorly than the humeral head of the bare hand at the initial position and approximately 2.5 mm inferiorly during the maximum abduction of the GH joint (Table 1 and Figure 3). No correlation was observed between the two groups concerning the change in SI-translated position depending on the shoulder abduction angle (R2 = 0.329; p = 0.273).
In the stick hand, the humeral head was more anterior and more superior to the bare hand until the abduction angle reached 40°. Then, it was located posterior and inferior from 50° to the maximum abduc- tion. The AP and SI translations were approximately 4.5~5.0 mm in the initial position to maximum abduction in the stick hand. Alternatively, the bare hand moved less than the stick hand by approximately 0.5~ 1.0 mm (Figure 3).
2. Scapular rotation
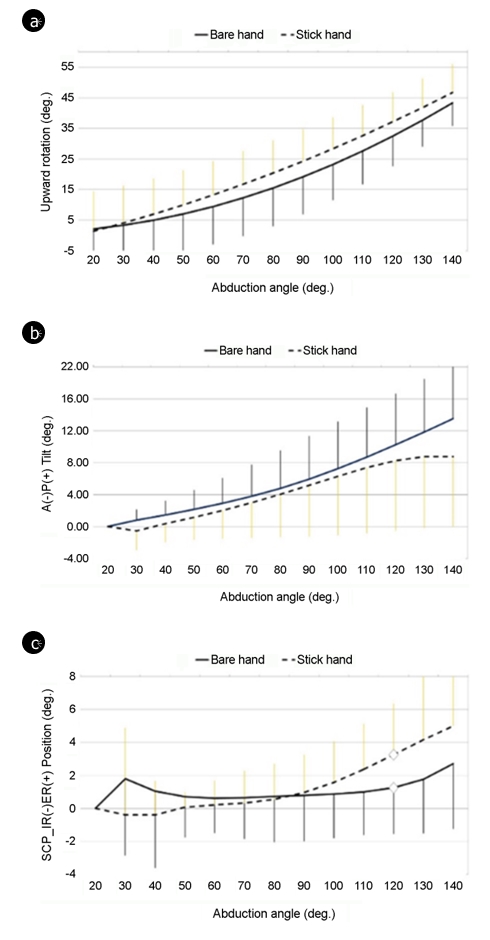
The average initial position of the scapula in both groups was 1~2° upward position relative to the origin. When the GH joint was at the maximal abduction of the scapula, the scapula was upward 43~46° relative to the initial position (Table 1). A correlation was found between the groups regarding changes in the translated position depending on the arm abduction angle (R2 = 0.995; p < 0.001) (Figure 4).
The initial position of the scapula in both groups was relative to the 0°. When the GH joint was at the maximal abduction of the scapula, the scapula was tilted posteriorly 8~13° relative to 0° (Table 1). A cor- relation between the groups was observed concerning changes in the translated position depending on the arm abduction angle (R2 = 0.978; p < 0.001) (Figure 4).
The initial position of the scapula in both groups was relative to 0°. When the GH joint was at the maximal abduction of the scapula, the scapula was externally rotated 2~5° relative to 0° (Table 1). In the stick hand, the humeral head was more internally rotated than the bare hand until the abduction angle reached 80°. Then, it was inversely positioned after the abduction angle reached 90°. When the scapula externally rotated 120° a statistically significant difference was observed between the groups (p < 0.05). In addition, a correlation between the groups was found concerning changes in the translated position depending on the arm abduction angle (R2 = 0.692; p = 0.009).
3. Scapulohumeral rhythm ratio
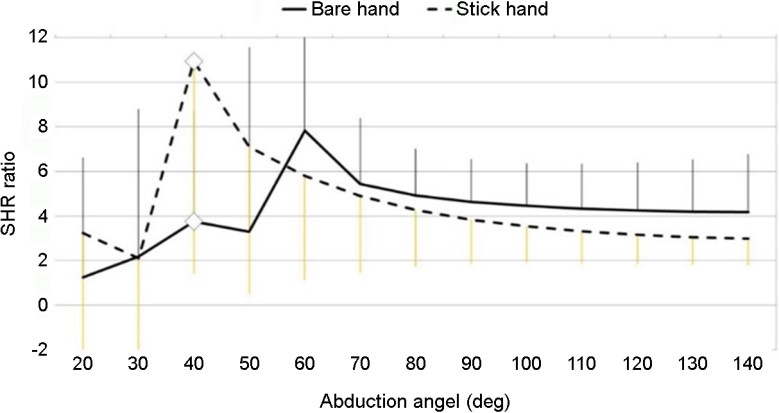
When the SHR was 40°, a statistically significant difference between the two groups was found (p < 0.05) (Figure 5). More humerus motion in the stick hand was observed than that in the bare hand until the abduction angle reached 50°. Then, it was inversely positioned after the abduction angle reached 60°. No correlation between the groups was observed regarding changes in the translated position depending on the arm abduction angle (R2 = 0.173; p = 0.572) (Figure 5).
This study was conducted to analyze the arthrokinematic movement of the shoulder joints with external loads through the equipment used in ice hockey athletes using the 3D-2D model registration technique. We assumed that movement of the humerus with an unstable contact basis through scapula plane abduction along with external load by an ice hockey stick would affect the joints. Compared with the bare hand, the humerus of the stick hand moved from the anterior aspect to the posterior aspect and from the superior aspect to the inferior aspect, and the scapula was rotated upward, tilted from anterior to posterior, and the SHR showed a tendency to decrease compared with that in the initial period.
In this study, humeral AP and SI translations were not statistically significantly different, but the movement of the humeral head could be predicted by the difference in displacement depending on the presence or absence of the stick. The humeral AP translation started with an anteriorly positioned humeral head at the initial movement when the stick was lifted, and the abduction movement of the humerus advanced to its original position. In the humeral SI translation, compared with the initial position of the humeral head, the stick hand started in a superior position compared with that of the bare hand that showed inferior movements throughout the abduction movement. Bey, Kline, Zauel, Lock & Kolowich (2008) and Matsuki et al. (2012) have reported a movement in the inferior direction before the superior movement of the humeral head when performing arm abduction. Additionally, Nishinaka et al. (2008) have reported a translation of only 1.7 mm in the superior direction. Therefore, we think that factors influencing the dynamic stability when humeral elevation changes are due to the muscles of the GH joint and shoulder girdle that are activated depending on the angle of the shoulder. Pratt (1994) and Kapandji (1964) have reported that the coupling of the deltoid-supraspinatus is important at the beginning of humeral elevation, and Lee and An (2002) have reported that the activation of the deltoid was increased up to 60° during shoulder abduction. The results of this study on the bare hand showed a pattern similar to that of humeral SI translation in the studies by Bey et al. (2008) and Matsuki et al. (2012). However, we believe that the continuous inferior movement observed in the stick hand during the initial abduction of the shoulder may be the pre-contraction of the deltoid muscle. In addition, no significant difference in the correlation of the humerus translation was found between hands with and without sticks, but it was observed that the relative position of the humeral angle was reversed from 40°. This suggests that stabili- zation of the humeral head due to the rotator cuffs, which is activated for posterior-inferior stability above 40°, after humeral movement through deltoid activation, affects AP and SI translation movements.
In this study, the scapular kinematics has a significant correlation with upward rotation (R2 = 0.995; p < 0.001), AP tilt (R2 = 0.978; p < 0.001), and internal to external rotation (R2 = 0.692; p = 0.009). Furthermore, it can be recognized that the scapula moves in a similar tendency with or without a stick. Internal to external rotation showed a tendency to be more erroneous in the stick hand than that in the bare hand after 90° and showed a significant difference at 120°. This result shows no significant difference in the dynamic stability of the scapula due to the contraction of the rotator cuff, but it can lead to a difference in the movement of the humerus on the side of the joint that has inherent instability.
In this study, the SHR ratio for the 40° abduction performed using the stick hand was significantly higher than that performed using the bare hand according to the statistical analyses (stick hand = 10.94± 9.52 vs. bare hand = 3.75±4.97), which was similar to the result of the previous study (Kon, Nishinaka, Gamada, Tsutsui & Banks, 2008). After the initial 30~50°, the ratio is consistent with the existing theory and progresses as the scapular movement increases. The length and weight of the hockey sticks used in this study were 165 cm and 535 g, re- spectively. The wrist was fixed, but a load of direction could be changed in contrast to what was performed in the study by Kon et al. (2008). Thus, the SHR ratio may be increased in the setting phase for the stabilization of the scapula. According to Inman et al. (1996), when the abduction of the shoulder occurs, there is a period when the humerus and scapula move through the "setting phase" approximately 0~30°, and the SHR is fixed at a 2:1 ratio (Inman et al., 1996). However, McClure, Michener, Sennett & Karduna (2001) have reported that the SHR ratio is not linear in an invasive study on scapula pinning. The previous study has reported that the SHR ratio may increase with the external load during abduction (McClure et al., 2001). Kon et al. (2008) have reported that the SHR ratio temporarily changes between 40° and 70° when arm abduction was performed with a dumbbell equivalent to an external load (Kon et al., 2008).
This study has several limitations. Because of the limited number of participants in the study, we could not compare the difference between the game position and the dominant hand of the participants. Since only a small sample of ice hockey players was examined, it cannot be generalized to them. Even though the temperature of the laboratory was maintained between 22℃ and 24℃, the humidity could not be controlled. Based on the results of this study, ice hockey players may be occurred overuse injury their arms holding the stick and may be weakened movement due to an imbalance of shoulder joints and muscles. Therefore, ice hockey coaches and athletic trainers should evaluate the player's body alignment as accurately as possible and conduct physical training based on an evaluation to ensure correct alignment and movement (i.e., flexion, extension, abduction, adduction, horizontal abduction, and horizontal adduction) of the shoulder. In future studies, examining the relationship between the game position of ice hockey players and the site of injury using an epidemiology approach will be necessary. Future studies should focus on developing equipment and/or injury prevention programs that can decrease the risk of injury based on epidemiological studies.
We analyzed the arthrokinematic movements of the shoulder joints with external loads using the equipment used by ice hockey athletes using the 3D-2D image registration technique. With arm loading with the stick, the humeral and scapular kinematics showed a significant correlation in the initial section of the SHR. Although these correlations might be difficult in clinical settings, it demonstrated that ice hockey athletes can lead to the movement difference of the scapulohumeral joints with inherent instability.
References
1. Agel, J. & Harvey, E. J. (2010). A 7-year review of men's and women's ice hockey injuries in the NCAA. Canadial Journal of Surgery, 53(5), 319-323. Bey, M. J., Kline, S. K., Zauel, R., Lock, T. R. & Kolowich, P. A. (2008). Measuring dynamic in-vivo glenohumeral joint kinematics: tech- nique and preliminary results. Journal of Biomechanics, 41(3), 711-714.
Google Scholar
2. Bey, M. J., Kline, S. K., Zauel, R., Lock, T. R. & Kolowich, P. A. (2008). Measuring dynamic in-vivo glenohumeral joint kinematics: tech- nique and preliminary results. Journal of Biomechanics, 41(3), 711-714.
Google Scholar
3. Dwyer, T., Petrera, M., Bleakney, R. & Theodoropoulos, J. S. (2013). Shoulder instability in ice hockey players: incidence, mechanism, and MRI findings. Clinics in Sports Medicine, 32(4), 803-813.
Google Scholar
4. Flik, K., Lyman, S. & Marx, R. G. (2005). American collegiate men's ice hockey: an analysis of injuries. The American Journal of Sports Medicine, 33(2), 183-189.
Google Scholar
5. Freedman, L. & Munro, R. R. (1966). Abduction of the arm in the scap- ular plane: scapular and glenohumeral movements: a roentgeno- graphic study. The Journal of Bone & Joint Surgery, 48(8), 1503-1510.
Google Scholar
6. Inman, V. T., Saunders, J. B. D. M. & Abbott, L. C. (1996). Observations of the Function of the Shoulder Joint. Clinical Orthopaedics and Related Research, 330, 3-12.
Google Scholar
7. Kapandji, I. A. (1964). Illustrated physiology of joints. Medical & Bio- logical Illustration, 14, 72-81.
Google Scholar
8. Kerr, Z. Y., Collins, C. L., Pommering, T. L., Fields, S. K. & Comstock, R. D. (2011). Dislocation/separation injuries among US high school athletes in 9 selected sports: 2005-2009. Clinical Journal of Sport Medicine, 21(2), 101-108.
Google Scholar
9. Koh, E. K., Weon, J. H. & Jung, D. Y. (2012). The comparison of electro- myographic ratio of serratus anterior and upper trapezius according to exercise position and shoulder flexion angle during scapular protraction exercises. Korean Journal of Sport Biomechanics, 22(2), 193-199.
Google Scholar
10. Kon, Y., Nishinaka, N., Gamada, K., Tsutsui, H. & Banks, S. A. (2008). The influence of handheld weight on the scapulohumeral rhythm. Journal of Shoulder and Elbow Surgery, 17(6), 943-946.
Google Scholar
11. Lee, B. K. (2009). The effect of atrophy of the inpraspinatus on strength and ROM in shoulder joint of male volleyball players. Korean Journal of Sport Biomechanics, 19(3), 549-555.
Google Scholar
12. Lee, B. K., Han, D. W. & Kang, K. H. (2007). Isokinetic performance and shoulder mobility in pro league woman volleyball players. Korean Journal of Sport Biomechanics, 17(4), 45-55.
Google Scholar
13. Lee, S. B. & An, K. N. (2002). Dynamic glenohumeral stability provided by three heads of the deltoid muscle. Clinical Orthopaedics and Related Research, 400, 40-47.
Google Scholar
14. Lee, Y. Y., Lee, C. H., Lee, S. M. & Kim, T. G. (2014). Etiologic factors of ice hockey injuries in Korean high school players. Pain Physician, 17, 747-754.
Google Scholar
15. Matsuki, K., Matsuki, K. O., Mu, S., Yamaguchi, S., Ochiai, N., Sasho, T., Sugaya, H., Toyone, T., Wada, Y., Takahashi, K. & Banks, S. A. (2011). In vivo 3-dimensional analysis of scapular kinematics: comparison of dominant and nondominant shoulders. Journal of Shoulder and Elbow Surgery, 20(4), 659-665.
Google Scholar
16. Matsuki, K., Matsuki, K. O., Yamaguchi, S., Ochiai, N., Sasho, T., Sugaya, H., Toyone, T., Wada, Y., Takahashi, K. & Banks, S. A. (2012). Dynamic in vivo glenohumeral kinematics during scapular plane abduction in healthy shoulders. Journal of Orthopaedic & Sports Physical Therapy, 42(2), 96-104.
Google Scholar
17. McClure, P. W., Michener, L. A., Sennett, B. J. & Karduna, A. R. (2001). Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. Journal of Shoulder and Elbow Surgery, 10(3), 269-277.
Google Scholar
18. McKay, C. D., Tufts, R. J., Shaffer, B. & Meeuwisse, W. H. (2014). The epidemiology of professional ice hockey injuries: a prospective report of six NHL seasons. British Journal of Sports Medicine, 48(1), 57-62.
Google Scholar
19. Mölsä, J., Airaksinen, O., Näsman O. & Torstila, I. (1997). Ice hockey injuries in Finland: a prospective epidemiologic study. The American Journal of Sports Medicine, 25(4), 495-499.
Google Scholar
20. Mölsä, J., Kujala, U., Myllynen, P., Torstila, I. & Airaksinen, O. (2003). Injuries to the upper extremity in ice hockey: analysis of a series of 760 injuries. The American Journal of Sports Medicine, 31(5), 751-757.
Google Scholar
21. Mölsä, J., Kujala, U., Näsman, O., Lehtipuu, T. P. & Airaksinen, O. (2000). Injury profile in ice hockey from the 1970s through the 1990s in Finland. The American Journal of Sports Medicine, 28(3), 322-327.
Google Scholar
22. Moro-oka, T. A., Hamai, S., Miura, H., Shimoto, T., Higaki, H., Fregly, B. J., Iwamoto, Y. & Banks, S. A. (2007). Can magnetic resonance imaging-derived bone models be used for accurate motion meas- urement with single-plane three-dimensional shape registration? Journal of Orthopaedic Research, 25(7), 867-872.
Google Scholar
23. Nishinaka, N., Tsutsui, H., Mihara, K., Suzuki, K., Makiuchi, D., Kon, Y., Wright, T. W., Moser, M. W., Gamada, K., Sugimoto, H. & Banks, S. A. (2008). Determination of in vivo glenohumeral translation using fluoroscopy and shape-matching techniques. Journal of Shoulder and Elbow Surgery, 17(2), 319-322.
Google Scholar
24. Poppen, N. & Walker, P. (1976). Normal and abnormal motion of the shoulder. Journal of Bone & Joint Surgery, 58(2), 195-201.
25. Pratt, N. E. (1994). Anatomy and biomechanics of the shoulder. Journal of Hand Therapy, 7(2), 65-76.
Google Scholar
26. Tuominen, M., Stuart, M. J., Aubry, M., Kannus, P. & Parkkari, J. (2015). Injuries in men's international ice hockey: a 7-year study of the International Ice Hockey Federation Adult World Championship Tournaments and Olympic Winter Games. British Journal of Sports Medicine, 49(1), 30-36.
Google Scholar
27. Tuominen, M., Stuart, M. J., Aubry, M., Kannus, P., Tokola, K. & Parkkari, J. (2016). Injuries in women's international ice hockey: an 8-year study of the World Championship tournaments and Olympic Winter Games. British Journal of Sports Medicine, 50(22), 1406-1412.
Google Scholar
