Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Na Mi Yoon
Yeon Soon Seo
Yang-Hoon Kang
http://dx.doi.org/10.5103/KJSB.2016.26.2.153 Epub 2016 July 14
Abstract
Objective: The purpose of this study was to investigate the effects of joint mobilization on foot pressure, ankle moment, and vertical ground reaction force in subjects with ankle instability.
Method: Twenty male subjects (age, 25.38 ± 3.62 yr; height, 170.92 ± 5.41 cm; weight, 60.74 ± 9.63 kg; body mass index (BMI), 19.20 ± 1.67 kg/m2) participated and underwent ankle joint mobilization. Weight¬bearing distribution, ankle dorsi/plantar flexion moment, and vertical ground reaction force were measured using a GPS 400 and a VICON Motion System (Oxford, UK), and subsequently analyzed. SPSS 20.0 for Windows was used for data processing and paired t-tests were used to compare pre- and post-mobilization measurements. The significance level was set at α = .05.
Results: The results indicated changes in weight-bearing, ankle dorsi/plantar flexion moment, and vertical ground reaction force. The findings showed changes in weight-bearing distribution on the left (pre 29.51 ± 6.31 kg, post 29.57 ± 5.02 kg) and right foot (pre 32.40 ± 6.30 kg, post 31.18 ± 5.47 kg). There were significant differences in dorsi/plantar flexion moment (p < .01), and there were significant increases in vertical ground reaction forces at initial stance (Fz1) and terminal stance (Fz2, p < .05). Additionally, there was a significant reduction in vertical ground reaction force at midstance (Fz2, p < .001).
Conclusion: Joint mobilization appears to alter weight-bearing distribution in subjects with ankle instability, with resultant improvements in stability.
Keywords
Foot pressure Ankle moment Vertical ground reaction force Joint mobilization
Postural control is the process of continuously maintaining the center of gravity of the body on the ground (Yaggie & McGregor, 2002), and maintaining balance requires continuous regulation by the sen- sory, musculoskeletal, and central nervous systems (Shumway-Cook & Woollacott, 2006). Even when one is standing still and the force and moment imposed on the ground are balanced, a complex musculo- skeletal control process is at play, and this process of maintaining posture is referred to as the postural control system (Singh, 2005).
Ankle instability (AI) most commonly occurs in people with ankle sprains, and it is also common in people with a history of ankle sprain (Konradsen, 2002). Furthermore, despite treatment, 50% of those who have had an ankle sprain experience residual symptoms, such as chronic instability and synovitis. AI is a result of repeated ankle sprains and is characterized by symptoms of instability, such as a feeling of the ankle giving way (Hiller et al., 2011), which can manifest as epidemiological and functional impairment of the ankle. Soft tissue damage from liga- ment injury or fracture can lead to structural instability, and proprio- ceptive sensory impairment near the ankle joint can lead to AI. AI may also manifest as functional instability, such as excess eversion, functional impairment of the muscles, or a reduction in range of motion of the ankle joint. Changes in the feet create inefficient functional instability of the ankle, resulting in pathologic instability, lack of ankle motion and synovial fluid, and degenerative changes. Inefficient functional instability leads to loss of proprioception, difficulty with neuromuscular control, loss of strength, and reduced postural control (Hertal, 2002).
Mulligan's mobilization with movement (MWM) is a treatment tech- nique that can be used to improve dorsiflexion after an ankle sprain by incorporating postero-anterior gliding of the tibia on the talus during active dorsiflexion movement (Mulligan, 1999). An accelerated recovery without pain is generally associated with the MWM technique (Mulligan, 1993, 1999; Exelby, 1996). A study that examined the effects of MWM on mildly limited ankle dorsiflexion found that MWM is effective for improving symmetric weight-bearing and ankle dorsiflexion range of motion (ROM) (Vicenzino et al., 2001). Akbari et al. (2007) reported that conservative treatment, such as arch supports, which are currently used to treat chronic foot and ankle diseases in people with AI, has been effective in mitigating pain and improving function, and recently sug- gested that arch supports produce positive effects on the sensorimotor system, through which the neuromuscular function of the lower extre- mities could be enhanced. However, whether ankle stabilization acces- sories, such as corrective tape and arch supports, could reduce bunion formation and hammer toe deformity, reduce foot and back pain, and measurably improve balance capacity remains a controversial matter (Hertel et al., 2001; Kelaher et al., 2000). To resolve AI, the ankle muscles must be strengthened, muscular strength and ROM must be recovered through proprioception exercises, and functional training must be per- formed for motor recovery. Such functional rehabilitation constitutes an important step in preventing damage, and reduces pain and edema more effectively than surgical fixation (Scott, 2007); in particular, func- tional rehabilitation comprised of proprioceptive exercises has been reported to reduce re-injury of the ankle ligaments (Michael & Thomas, 2003). In this study, we applied ankle mobilization techniques to indi- viduals with AI and established hypotheses pertaining to foot pressure, which represents changes in body pressure, ankle joint moment, which represents intraarticular muscle activation, and vertical ground reaction force (GRF), which represents the reaction force to the moment and the ground. Then, we examined the effects of ankle articular mobilization on foot pressure, ankle joint moment, and vertical GRF in individuals with AI, in an attempt to provide basic data to assess clinical utility.
1. Subjects
We enrolled 20 male participants with AI who provided written con- sent. We did not explain the content, procedures, and anticipated effects of the study to the participants. The participants' general characteristics were determined using a body composition analyzer (InBody J05, Bio- space, USA). The inclusion criteria were as follows: normal individuals with no ambulatory problems from orthopedic surgery or dysfunction in the lower extremities, and those who could maintain independent standing for at least one minute. Individuals with a history of hyper- tension or diabetes, visual or vestibular dysfunction, or orthopedic dis- orders of the upper and lower extremities or the trunk were excluded from the study.
Patient characteristics are shown in Table 1. The mean age of the subjects was 25.38 ± 3.62 years with a mean height of 170.92 ± 5.41 cm, weight of 60.74 ± 9.63 kg, and body mass index (BMI) of 19.20 ± 1.67 kg/m2.
|
Characteristics |
Subjects |
|
Age
(years) |
25.38 ± 3.62 |
|
Height
(cm) |
170.92 ± 5.41 |
|
Weight
(kg) |
60.74 ± 9.63 |
|
BMI (kg/m2) |
19.20 ± 1.67 |
2. Study design
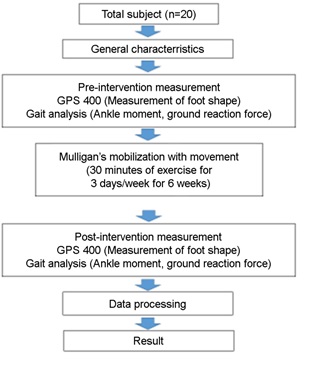
This study quantitatively assessed the effects of ankle articular mobili- zation on foot pressure, ankle moment, and vertical GRF, and compared the pre-intervention and post-intervention effects after treatment for 30 min/day for 3 days per week for 6 weeks (Figure 1).
3. Exercise methods
We administered the MWM technique (Figure 2) on 20 male partici- pants with AI. First, the patient was positioned supine on the treatment table with the ankle joint in a comfortable position. The calf was fixed to the treatment table using a belt while the talus was bound with another belt, making a loop that almost touched the floor. With the toes touching the ground, the clinician placed his or her heel within the loop in a standing position and moved the heel downward. This movement glided the talus posteriorly, enabling the ankle joint to glide posteriorly into dorsiflexion (Kaltenborn, 2007). After maintaining the posture for 10 seconds, the clinician reverted back to the starting position for a 5-second break, and repeated this 10 times (1 set) for a total of 6 sets (Colins et al., 2004; Vicenzino et al., 2006).
4. Measurement methods
1) Measurement of foot shape
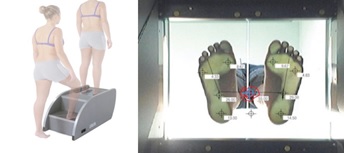
The GPS 400 (Global Postural System) was used to comprehensively analyze foot shape, and the PODATA device was used to analyze weight-bearing distribution, the proportion of foot pressure on the fifth metatarsal, and the proportion of foot pressure on the calcaneus. Foot pressure distribution was analyzed by installing the PODATA device and Philips cameras on the GPS, which automatically calculated the ratio of the maximum length of the forefoot to the minimum length of the midfoot. Recently, foot pressure tests have been used to diagnose foot deformities using quantitative data. For our study, foot pressure was first measured while the participant maintained standing balance, facing forward, with the legs spread apart 30°, and the limits of stability were measured while the participant maintained standing balance using an ankle strategy to shift their center of gravity to the maximum range. The unit of measurement was % kg for the weight on each foot (Figure 3).
2) Measurement of ankle joint moment and vertical GRF
First, we performed the body measurements required for data analysis during static examinations, including height, weight, BMI, and length of both lower limbs. Ankle moment was measured 3 times as the participant walked 10 m, and vertical GRF was measured via an inverse dynamic method using two force platforms installed on the floor. All data were statistically processed and averaged to compare pre-intervention and post-intervention measurements. For static and dynamic tests, 3-dimensional kinematic gait changes were measured using a 6-camera motion analysis system (120 Hz, VICON Motion Systems Ltd., Oxford, UK) on a PC in which VICON workstation software (Oxford Metrics, Oxford, UK) had been installed. After adjusting for the potential errors of the cameras prior to the test, markers were attached to the main joints and muscles of the hip and lower limbs while the participant stood still on the force platforms in order to measure the position of each joint on the computer monitor connected to the VICON optical motion capture system. The markers were round with a diameter of 1.4 cm. The measurement values were computed using the VICON Plug¬In-Gait model (Figure 4).
5. Analysis method
All data were analyzed via SPSS for Windows version 20.0 statistical program (IBM Corp., Armonk, NY, USA). We used descriptive statistics to examine the general characteristics of the participants and pre- and post-intervention foot pressure, and used paired t-tests to examine the significance of the differences between pre- and post-intervention ankle moment and vertical GRF. The significance level α was set to 0.05.
1. Comparison of pre-intervention and post-intervention weight distribution while standing
Table 2 shows the comparison of pre- and post-intervention weight distribution on each foot while standing. Prior to the intervention, the weight distribution on the left and right foot were 29.51 ± 6.31 kg and 32.40 ± 6.30 kg, respectively, while those after the intervention were 29.57 ± 5.02 kg and 31.18 ± 5.47 kg, respectively. Prior to the inter- vention, the pressure on the fifth metatarsal of the left and right foot was 42.85 ± 9.60% kg and 35.37 ± 13.34% kg, respectively, while after the intervention, it was 41.58 ± 9.97% kg and 36.29 ± 13.38% kg, respectively. Prior to the intervention, pressure on the left and right calcaneus was 38.03 ± 14.33% kg and 45.93 ± 17.75% kg, respectively, while after the intervention, it was 41.28 ± 12.05% kg and 48.03 ± 11.95% kg, respectively.
|
|
Pre |
Post |
|
Weight
on the left foot (kg) |
29.51 ± 6.31 |
29.57 ± 5.02 |
|
Weight
on the right foot (kg) |
32.40 ± 6.30 |
31.18 ± 5.47 |
|
%
weight distribution of the left foot on the 5th metatarsal (% kg) |
42.85 ± 9.60 |
41.58 ± 9.97 |
|
%
weight distribution of the left foot on the calcaneus (% kg) |
38.03 ± 14.33 |
41.28 ± 12.05 |
|
%
weight distribution of the right foot on the 5th metatarsal (% kg) |
35.37 ± 13.34 |
36.29 ± 13.38 |
|
%
weight distribution of the right foot on the calcaneus (% kg) |
45.93 ± 17.75 |
48.03 ± 11.95 |
2. Comparison of pre-intervention and post-intervention ankle joint sagittal moment
Table 3 shows the comparison of pre- and post-intervention ankle joint sagittal moments. The ankle plantar flexion moments before and after the intervention were 0.10 ± 0.08 Nm/kg and 0.19 ± 0.19 Nm/ kg, respectively, showing a significant difference between the pre- and post-intervention values (p < .01). The ankle joint dorsiflexion moments before and after the intervention were 1.21 ± 0.31 Nm/kg and 1.38 ± 0.18 Nm/kg, respectively, showing no significant difference between the pre- and post-intervention values. However, there was a significant difference between pre- (1.35 ± 0.13 Nm/kg) and post-intervention ankle joint sagittal moment ROM (1.58 ± 0.23 Nm/kg) (p < .01).
|
|
Pre |
Post |
t |
p |
|
Ankle
plantar flexion |
0.10 |
0.19 |
-3.834 |
.002* |
|
Ankle
dorsiflexion |
1.21 |
1.38 |
-1.831 |
.088 |
|
Ankle dorsi/Plantar
flexion |
1.35 |
1.58 |
-4.109 |
.001* |
3. Comparison of pre-intervention and post-intervention medial and lateral GRF
Table 4 shows the changes in each group in medial and lateral GRF. The peak medial GRFs (FML1) at the midpoint of the loading response, during which shock absorption occurs at first contact with the ground, were 3.65 ± 1.66% body weight (BW) and 4.16 ± 1.74% BW, before and after the intervention, respectively. The peak lateral GRFs (FML2) during terminal stance phase, which maintain the stability of the foot and help the foot to propel the body forward, were 14.66 ± 4.66% BW and 19.95 ± 3.81% BW, before and after the intervention, respectively. These findings indicate that the peak lateral GRF increased after the intervention (p < .01).
|
|
Pre |
Post |
t |
p |
|
FML1 max |
3.65 ± 1.66 |
4.16 ± 1.74 |
-.832 |
.419 |
|
FML2 max |
14.66 ± 3.32 |
19.95 ± 3.81 |
-3.454 |
.004* |
4. Comparison of pre-intervention and post-intervention vertical GRF
Table 5 shows the changes in each group in vertical GRF. In the initial stance phase (Fz1), during which the body’s center of gravity rapidly drops and weight accelerates, the pre- and post-intervention vertical GRFs were 105.57 ± 5.72% BW and 111.50 ± 8.91% BW, respectively, while those at midstance (Fz0), during which the body advances over the stationary foot and the center of gravity rises upward, were 83.33 ± 3.68% BW and 69.69 ± 6.18% BW, respectively. In addition, the pre- and post-intervention vertical GRFs in terminal stance (Fz2), during which the body's center of gravity rises upward, were 104.66 ± 5.22% BW and 111.25 ± 7.76% BW, respectively. There was a significant difference between the pre- and post-intervention vertical GRFs, such that vertical GRFs increased at initial contact (Fz1) and terminal stance (Fz2) after the intervention (p < .05), while markedly declining during midstance (p < .001) after the intervention.
|
|
Pre |
Post |
t |
p |
|
Fz1 |
105.57 ± 5.72 |
111.50 ± 8.91 |
-2.302 |
.037* |
|
Fz0 |
83.33 ± 3.68 |
69.69 ± 6.18 |
7.451 |
.000** |
|
Fz2 |
104.66 ± 5.22 |
111.25 ± 7.76 |
-2.416 |
.030* |
The body uses various strategies to maintain balance during per- turbation, and the selection of the strategy depends on the specific situation. In addition, the sequencing of muscle activation varies widely depending on the properties and capacities of the selected strategy, and responses differ in accordance with the position of the feet on the ground, such as whether foot movement is free or hindered, the basal plane is large or small, or balance is perturbed (Shumway-Cook & Woollacott, 2006). The feet are the point of contact between the body and the ground during gait, and the resulting sensory information created by this contact is delivered to the central nervous system, and then used to maintain the body and to perform body movements (Giulio, Maganaris, Baltzopoulos, & Loram, 2009). Based on the pressure distributed along the soles, the feet send sensory information pertaining to the body and the ground to the nervous system, promoting sensory input for postural maintenance (Menz et al., 2005). Excessive asymmetry resulting from foot deformities produces trunk and spinal deviations, as well as asymmetries in muscle strength. Asymmetric muscle activity may induce asymmetric muscle development due to inefficient use, and foot deformities could also influence static and dynamic posture and therefore the balance of the lower limbs and trunk (Schamberger, 2002). Foot pressure represents the proportion of pressure on the first metatarsalphalangeal (MTP) joint, fifth MTP joint, and calcaneus, and the analysis of foot pressure enables an examination of the factors that cause foot injury and deformity. In addition, maximum pressure in static stance can be measured to examine the relationship between foot deformity and foot pressure, enabling the assessment of inversion and eversion strength of the foot, which may influence ankle stability (Pitei et al., 1999). According to the findings of the present study, the weight-bearing distribution of the feet was asymmetrical in standing, with pre-intervention weight on the left and right equaling 29.51 ± 6.31 kg and 32.40 ± 6.30 kg, respectively. After the intervention, the weight on the left and right foot were found to be 29.57 ± 5.02 kg and 31.18 ± 5.47 kg, respectively. Prior to the intervention, the pressure on the fifth meta- tarsal of the left and right foot were 42.85 ± 9.60% kg and 35.37 ± 13.34% kg, respectively, while those after the intervention were 41.58 ± 9.97% kg and 36.29 ± 13.38% kg, respectively. Prior to the intervention, calcaneal pressure on the left and right foot were 38.03 ± 14.33% kg and 45.93 ± 17.75% kg, respectively. Joint position sense is more de- pendent on muscle receptors than on ligament or joint receptors, so these results seem to indicate asymmetric activation of the muscles around the ankle of one foot due to asymmetric weight load. Further- more, the MWM technique seems to have improved the AI caused by weakened muscles and soft tissues around the ankle, resulting in changes in weight distribution, in agreement with our hypothesis. In addition, increased inversion force on the ankle aggravates AI while bearing weight, but the MWM technique is presumed to play a positive role in standing balance by improving ankle stability and the reaction speed of the peroneal muscles, leading to changes in the proportion of foot pressure on the fifth metatarsal and stimulation of the proprio- ceptors of the gastrocnemius and tibialis anterior.
David et al. (2013) emphasized the fact that patients with AI display eccentric contractions of the invertor and evertor muscles, suggesting that individuals with AI have reduced dorsiflexion compared to people with normal ankle stability. Hertel et al. (2000) reported that deficiencies in ankle muscle strength and position sense, reductions in peroneal muscle reaction time, balance deficits, and reductions in ankle dorsi- flexion ROM are associated with AI. AI is characterized by symptoms such as continuous ankle injury caused by repeated abnormal inversion forces on the foot, functional instability and muscular weakness, and delays in muscle reaction time (Hertel, 2002). These symptoms may result in weakness, fatigue, and pain in specific areas, such as the feet and legs, and AI may induce several postural symptoms and disor- ders (Scott et al., 2007). Inaccurate alignment of each area of the foot deforms the heel and impairs balance, which leads to asymmetric dis- tribution of body weight on the soles via the hip, knee, and ankle joints, ultimately causing additional symptoms (Defrin et al., 2005). In the pre- sent study, pre- and post-intervention plantar flexion moment values were 0.10 ± 0.08% BW and 0.19 ± 0.13% BW, respectively, exhibiting a significant difference (p < .01). On the other hand, there was no significant difference between pre- and post-intervention dorsiflexion moments (1.21 ± 0.31% BW and 1.38 ± 0.18% BW, respectively). There was a significant difference between pre- and post-intervention ankle joint sagittal moment ROM (1.35 ± 0.13% BW and 1.58 ± 0.23% BW, respectively) (p < .01). In terms of medial and lateral GRF, the peak medial GRFs before and after the intervention were 3.65 ± 1.66% BW and 4.16 ±.16% BW, respectively, while the peak lateral GRFs before and after the intervention were 14.66 ± 3.32% BW and 19.95 ± 3.81% BW, respectively, showing a significant increase in peak lateral GRF after the intervention (p < .01). In order to reduce AI, the functional motions of the ankle joints should be emphasized with particular attention to the dynamics of neuromuscular control that stabilize the ankles. The hypo- thesis of this study was accepted since the reinforcement of ankle proprioception via the MWM technique increased ankle stability by increasing plantar flexion moment, ankle ROM, and lateral GRF during weight-bearing. Hence, we expect that increased ankle stability will result in the effective delivery of accurate proprioceptive information, preventing ankle injury during unpredictable situations or due to changes in the environment.
McKeon et al. (2008) performed balance training with adults with AI and tested static postural control. Their findings indicated that there were no significant differences between pre-training and post-training variables pertaining to the center of pressure with the exception of a reduction in the speed of the antero-posterior movement of the center of gravity, which they reported was due to the fact that sufficient visual feedback was provided to assist postural control. Therefore, they re- ported that visual input can compensate for muscular fatigue of the limbs in postural control, and that visual input assisted with compen- sation in order to maintain postural stability. Hopkins et al. (2012) exa- mined the relationship between balance and proprioception and weight load in adults with AI and found that the center of gravity was dis- placed laterally during the stance phase of gait, and that the center of gravity was displaced anterolaterally compared to normal individuals during single leg balance on a force plate. While standing still, ground reaction force or center of gravity is usually used to maintain static balance, and the characteristics related to the displacement of the center of gravity are used to infer the neurological and dynamic mech- anisms of postural control (Mettler et al., 2015). According to the results of the present study, at initial stance (Fz1), during which the body's center of gravity rapidly drops and weight accelerates, the pre- and post-intervention vertical GRFs were 105.57 ± 5.72% BW and 111.50 ± 8.91% BW, respectively, and those at midstance (Fz0), during which the body advances over the stationary foot and the center of gravity rises upward, were 83.33 ± 3.68% BW and 69.69 ± 6.18% BW, respec- tively. In addition, the pre- and post-intervention vertical GRF at terminal stance (Fz2), during which the body accelerates inferiorly, were 104.66 ± 5.22% BW and 111.25 ± 7.76% BW, respectively. There was a signifi- cant difference between pre- and post-intervention vertical GRFs, where vertical GRF increased at initial stance (Fz1) and terminal stance (Fz2) after the intervention (p < .05), while markedly declining in the mid- stance phase after the intervention (p < .001). The fact that the vertical GRFs significantly increased during the initial stance phase (Fz1) and terminal stance phase (Fz2) after administering the MWM technique indicates that balance maintenance during alternating antero-posterior perturbation is dependent on the alternating activation of the tibialis anterior and medial gastrocnemius, where the medial gastrocnemius is activated before the body falls anteriorly after passing the vertical line, and the tibialis anterior is activated before the body has risen posteriorly. In addition, the greater the weight load, the more the proprioceptive receptors in the skin and muscles near the feet and ankles are stimu- lated, increasing postural stability, which confirms our hypothesis. Fur- thermore, the fact that there was a significant change during midstance (Fz0) following intervention shows that the blockade of sensory feed- back via visual input resulted in greater reliance on proprioceptive sensory input, and improved ankle stability led to more symmetric distribution of body weight on the soles of the feet, distributing the body weight through the hip, knee, and ankle joints, and thereby leading to a marked decrease in vertical GRF. It is difficult to generalize the findings of this study to all individuals with AI, and we are limited in the interpretation of our results because we did not conduct an EEG test on the ankle muscles while measuring foot pressure, ankle joint moment, and vertical GRF. These limitations should be addressed in future studies.
References
1. Akbari, M., Mohammadi, M. & Saeedi, H. (2007). Effects of rigid and soft foot orthoses on dynamic balance in females with flat foot. Medical Journal of the Islamic Republic of Iran, 21, 91-97.
Crossref
Google Scholar
2. Collins, N., Teys, P. & Vicenzino, B. (2004). The initial effects of a Mulligan's mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains. Manual Therapy, 9(2), 77-82.
Crossref
Google Scholar
PubMed
3. David, P., Halimi, M., Mora, I., Doutrellot, P. L. & Petitjean, M. (2013). Isokinetic testing of evertor and invertor muscles in patients with chronic ankle instability. Journal of Applied Biomechanics, 29(6), 696-704.
Crossref
Google Scholar
PubMed
4. Defrin, R., Benyamin, S. B., Aldubi, R. D. & Pick, C. G. (2005). Conservative correction of leg-length discrepancies of 10 mm or less for the relief of chronic low back pain. Archives of Physical Medicine and Rehabilitation, 86(11), 2075-2080.
Crossref
Google Scholar
PubMed
5. Exelby, L. (1996). Peripheral mobilisations with movement. Manual Therapy, 1(3), 118-126.
Crossref
Google Scholar
PubMed
6. Giulio, I. D., Maganaris, C. N., Baltzopoulos, V. & Loram, I. D. (2009). The proprioceptive and agonist roles of gastrocnemius, soleus and tibialis anterior muscles in maintaining human upright posture. The Journal of Physiology, 587(10), 2399-2416.
Crossref
Google Scholar
7. Hertel, J. (2000). Functional instability following lateral ankle sprain. Sports Medicine, 29(5), 361-371.
Crossref
Google Scholar
PubMed
8. Hertel, J., Denegar, C. R., Buckley, W. E., Sharkey, N. A. & Stokes, W. L. (2001). Effect of rearfoot orthoses on postural control in healthy participants. Journal of Sports Rehabilitation, 10, 36-47.
Crossref
9. Hertel, J. (2002). Functional anatomy, pathomechanics and pathophysi- ology of lateral ankle instability. Journal of Athletic Training, 37, 364-375.
Crossref
Google Scholar
PubMed
10. Hiller, C. E., Kilbreath, S. L. & Refshauge, K. M. (2011). Chronic ankle in- stability: evolution of the model. Journal of Athletic Training, 46(2), 133-141.
Crossref
Google Scholar
PubMed
11. Hopkins, J. T., Coglianese, M., Glasgow, P., Reese, S. & Seeley, M. K. (2012). Alterations in evertor/invertor muscle activation and center of pressure trajectory in participants with functional ankle instability. Journal of Electromyography and Kinesiology, 22(2), 280-285.
Crossref
Google Scholar
PubMed
12. Kaltenborn, F. M., Evjenth, O., Kaltenborn, T. B., Morgan, D. & Vollowitz, E. (2014) Manual Mobilization of the Joints, Vol. 1: The Extremities, 8th Edition, Orthopedic Physical Therapy Products.
Crossref
13. Kelaher, D., Mirka, G. A. & Dudziak, K. Q. (2000). Effects of semi-rigid arch-support orthotics: an investigation with potential ergonomic implications. Applied Ergonomics, 31(5), 515-522.
Crossref
Google Scholar
PubMed
14. Konradsen, L. (2002). Factors Contributing to Chronic Ankle Instability: Kinesthesia and Joint Position Sense. Journal of Athletic Training, 37(4), 381-385.
Crossref
Google Scholar
PubMed
15. Menz, H. B., Morris, M. E. & Lord, S. R. (2005). Foot and ankle char- acteristics is associated with impaired balance and functional ability in older people. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 60(12),1546-1555.
Crossref
16. Mettler, A., Chinn, L., Saliba, S. A., Mckeon, P. O. & Hertel, J. (2015). Balance training and center of pressure location in participants with Chronic ankle instability. Journal of Athletic Training, 50(4), 343-349.
Crossref
Google Scholar
PubMed
17. Michael, D. & Thomas, D. (2003). Prevention and treatment of ankle sprain in athletes. Sports Medicine, 33 (15), 1145-1150.
Crossref
Google Scholar
PubMed
18. McKeon, P. O. & Hertel, J. (2008). Systematic review of postural control and Lateral ankle instability, part II: is balance training clinically effective. Journal of Athletic Training, 43(3), 305-315.
Crossref
Google Scholar
PubMed
19. Mulligan, B. R. (2003) Manual Therapy: NAGS SNAGS MWMS ets, 6th Edition, Orthopedic Physical Therapy Products.
Crossref
20. Mulligan, B. R. (1993) Mobilisations with movement (MWM'S). The Journal of Manual and Manipulative Therapy, 1(4), 154-156.
Crossref
Google Scholar
21. Pitei, D. L., Lord, M., Foster, A., Wilson, S., Watkins, P. J. & Edmonds, M. E. (1999). Plantar pressures are elevated in the neuroischemic and the neuropathic diabetic foot. Diabetes Care, 22, 1966-1970.
Crossref
Google Scholar
PubMed
22. Schamberger, W., Fredric, T. S. & Webster, T. (2002). The Malalignment Syndrome. Edinburgh, Churchill Living stone.
Crossref
23. Singh, N. B. (2005). Evaluation of circumferential ankle pressure as an ergonomic intervention to maintain balance perturbed by localized muscular fatigue of the ankle joint. Master of Science In Industrial and Systems Engineering.
Crossref
Google Scholar
24. Scott, G., Menz, H. B. & Newcombe, L. (2007). Age-related in foot structure And function. Gait Posture, 26(1), 68-75.
Crossref
Google Scholar
PubMed
25. Yaggie, J. A. & McGregor, S. J. (2002). Effects of isokinetic ankle fatigue on the maintenance of balance and postural limits. Archives of Physical Medicine Rehabilitation, 83, 224-228.
Crossref
Google Scholar
PubMed
26. Vicenzino, B., Branjerdporn, M., Teys P. & Jordan, K. (2006). Intial changes in posterior talar glide and dorsiflexion of the ankle after mobili- zation with movement in individuals with recurrent ankle sprain. Journal of Orthopaedic & Sports Physical Therapy, 36(7), 464-471.
Crossref
Google Scholar
27. Vicenzino, B., Prangley, I. & Martin, D. (2001). The initial effect of two Mulligan mobilisation with movement treatment techniques on ankle dorsiflexion. In Australian Conference of Science and Medicine in Sport. Sports Medicine Australia.
Crossref
Google Scholar
