Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Que Tae Park
Suk Bum Kim
David O'Sullivan
http://dx.doi.org/10.5103/KJSB.2019.29.2.105 Epub 2019 July 06
Abstract
Objective: The main purpose of this study was to investigate the effects of wearing an ankle weight belt while performing gait in water by focusing on the effect of using ankle weights have on the gait kinematics and the muscle activities for developing optimum training strategies.
Method: A total of 10 healthy male university students were recruited for the study. Each participant was instructed to perform 3 gait conditions; normal walking over ground, walking in water chest height, and walking in water chest height while using ankle weights. All walking conditions were set at control speed of 4 km/h ± 0.05 km/h. The depth of the swimming pool was at 1.3 m, approximately chest height. The motion capture data was recorded using 6 digital cameras and the EMG was recorded using waterproof Mini Wave. From the motion capture data, the following variables were calculated for analysis; double and single support phase (s), swing phase (s), step length (%height), step rate (m/s), ankle, knee, and hip joint angles (°). From the electromyography the %RVC of the lower limb muscles medial gastrocnemius, rectus femoris, erector spinae, semitendinosus, tibialis anterior, vastus lateralis oblique was calculated.
Results: The results show significant differences between the gait time, and step length between the right and left leg. Additionally, the joint angular velocities and gait velocity were significantly affected by the water resistance. As expected, the use of the ankle weights increased all of the lower leg maximum muscle activities except for the lower back muscle.
Conclusion: In conclusion, the ankle weights can be shown to stimulate more muscle activity during walking in chest height water and therefore, may be useful for rehabilitation purposes.
Keywords
Ankles weights Aqua treadmill Aqua-walking Rehabilitation
Aquatic exercise therapy has been shown to be an effective exercise method to maintain health and help rehabilitation in diverse groups such as patients with arthritis, hemiplegic, injured athletes, and the elderly. By applying the body movement which is free from the stresses of exercising on ground, water has the merit that it enables more free movement all while maintaining water resistance which helps build and maintain muscle (Koury, 1996).
In Korea, interest in aquatic exercises and therapy have been rapidly increasing since the 1990s, focusing mainly in the welfare centers for the disabled and the older (over 65 years of age) population (Kim, Moon, & Yu, 2014). Recently, several researchers have conducted various studies on the effect of underwater rehabilitation exercise, and reported on the positive effect of improving physical strength and walking ability through aquatic exercise (Driver, O'Connor, Lox, & Rees, 2004; Nam, Kim, & Cho, 2004; Nielsen et al., 1996).
There have been numerous published articles highlighting the physical improvements such as the increase in endurance of people with disabilities such as arthritis (Danneskiold-Samsøe, Lyngberg, Risum, & Telling, 1987; Svedenhag & Seger, 1992), and low back pain (An, 2003), due to the overall increase in physical fitness, muscular strength, balance, and flexibility. Additional studies have further reported improvements of strength, balance and body fat loss (Kim, 1998), improvements in muscle symmetry (Wilder, 1993), increased blood circulation, and increase of muscle strength and improvement in cardiovascular systems for the elderly (Kim & Choi, 2006). Furthermore, studies have even shown that aqua therapy and walking in water can improve the gait pattern of patients suffering from a stroke (Chung, Kim, & Chun, 2011). Training in water was reported to help the patient have more free movement which translated to increases in joint ranges The effect of the water's buoyancy is also shown to help hemiplegic patients by affecting their gait pattern positively (Park et al., 2014), and increases their walking speed (Lee, Hyung, & Shim, 2009) and other related factors such as longer strides and more stability. Many studies have reported the effect of exercise on physical changes before and after exercise in aqua therapy rehabilitation exercises. However, these studies have a limitation of not being able to comment on the mechanism of physical changes that occur in the water.
In other words, if we can know how the motion in the water affects the body movement kinematics (i.e. mechanics) in detail, it will be useful for designing more suitable aquatic exercise program according to the patient's condition and thus increase the effectiveness of the exercise therapy. In order to confirm the changes in movement kinematics in water, Ryu and Kim (2008) compared the underwater walking posture with increasing weight ratio using a camera capable of underwater photographing. In a step up, Kim et al. (Kim, Moon, & Yu, 2014) analyzed gait pattern according to changes of water depth by underwater cameras. However, there have been difficulties in conducting empirical experiments to confirm various movement kinematics in water due to limitations of access to facilities fitted with underwater cameras and waterproof electromyography systems, which have only recently been developed for research.
In this study, the primary aim was to investigate the change in kinematics and muscle activity by using cameras and an electromyography system. The secondary aim was to investigate the effects of walking on walking under the following 3 conditions; walking over ground, walking in water up to chest height, and walking in water with an ankle weights with water chest height.
1. Participants
This study was conducted after approval of Institutional Review Board (IRB) (KYU-2018-116-01) of the University. The participants were 10 university students in the twenties. The participant's data collection only began after fully explaining the purpose of the study and the procedure of the experiment, the participant signed the IRB approved consent form. The participant demographics are shown in Table 1.
|
No. of participants |
Age (yrs) |
Height (cm) |
Weight (kg) |
|
|
Average ± Standard deviation |
10 males |
24.10±1.60 |
170.30±4.88 |
78.60±5.74 |
2. Experimental equipment
1) Motion capture
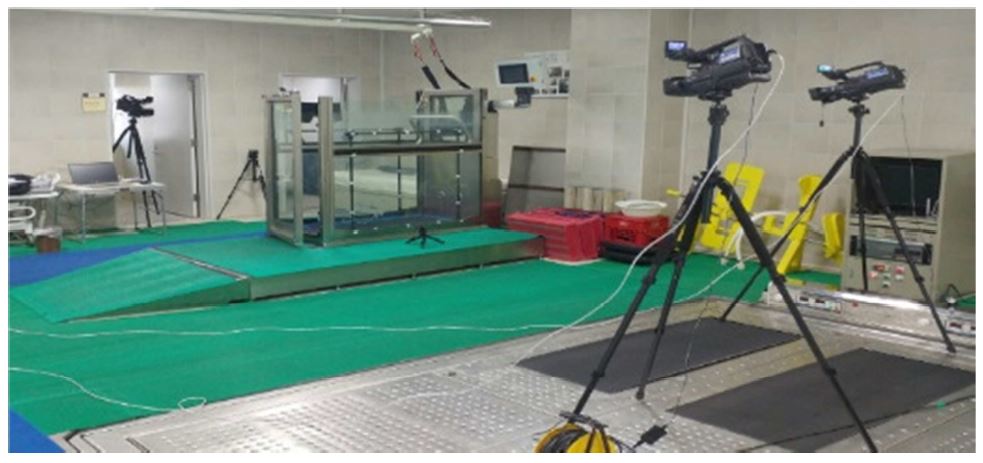
The motion capture equipment consisted of 6 digital video cameras and a control frame. The cameras recorded at 60 frames per second and a control frame (1 × 0.75 × 1 m) had points for digitization every 0.25 m along each of the 3 dimensions. Each recorded image was then imported into Kwon 3D XP for the calculation of the 3 dimensional coordinates and the calculation of the relative joint angles of each of the participants during each trial. The equipment set up is shown in Figure 1.
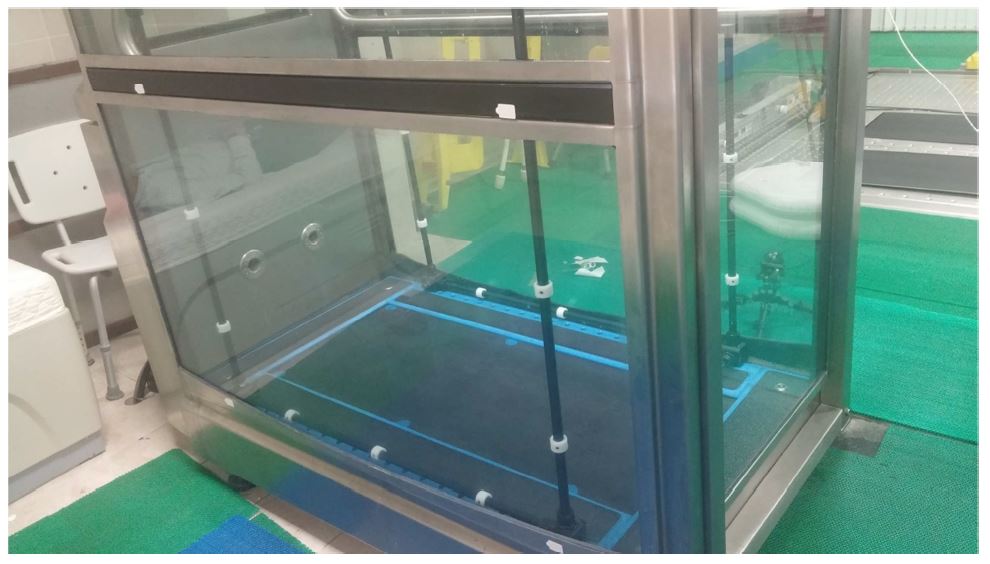
2) Underwater treadmill and ankle weight
The underwater treadmill (Aquabilt Pat302, USA) used for the experiment is shown in the Figure 2. The ankle weight used was 1 kg.
3) Wireless underwater electromyography system
The electromyography signals from the muscles were collected by the Mini Wave Waterproof System (Cometa, Italy). The measurement and recording software is provided by Cometa which has the option for export to C3D for analysis through Visual3D software (ver. 5.01, C-Motion Inc. USA).
3. Testing procedure
After an oral explanation and signing the University Hospital IRB consent form, the participants were asked to practice the underwater walking exercise for about 5 minutes and then reflective markers were attached. Each participant was instructed to walk at a preferred walking speed for the three conditions, walking over-ground, walking in the water, and walking in the water with the ankle weights. Each participant was filmed for 3 minutes and 10 consecutive steps were selected for analysis. Prior the data collection the control frame (2 × 2 × 3 m) was recorded by the six cameras (60 frames / sec) to set up the absolute coordinates where the underwater treadmill was to be recorded. The control frame was the removed and the data collection begun.
4. Data processing and analysis
1) Video analysis procedure
(1) Control frame and reference axis
In order to set the coordinates, a control point frame with a length of 1 m, a height of 0.75 m, and a height of 1 m is used as a reference for the global coordinates. The left mediolateral direction was set as the X axis and the vertical direction is set as the Z axis, and the Y axis was set as the cross product of the two vectors. All the major joint centers for the hip, knee and ankle, and segments for the lower body extremities were estimated using the Helen Hayes Marker set.
(2) Calculating the 3D coordinates
The three-dimensional coordinates were calculated using the DLT (Direct Linear Transformation method) method. Sixteen DLT coefficients were calculated from the two-dimensional coordinate values of the control points acquired from the six cameras and the position information on the reference plane. All the points are interpolated using a cubic spline function at constant sampling frequency of 125 Hz. Noise and artifacts affecting the quality of the data, such as skin movement and digitizing errors are smoothened using a 2nd order low-pass Butterworth filter.
(3) Gait phases and events
The right heel contact (RHC) is the moment when the right heel touches the ground, the left toe-off (LTO) when the left toe is raised from the ground, and the left heel contact (LHC) when the left heel comes in contact with the ground. The right toe-off (RTO) were defined as the time when the right toe is taken off the ground. The right support phase (s) or contact time is calculated from RHC to RTO and the left support phase (s) is from LTO to LHC. The swing time (s) is defined as the RTO to the RHC, and the LTO to the LHC. The step length (m) is defined as the distance from the left ankle position to the right ankle position during the stance phase. The step rate is the step length divide the time (m/s).
2) Electromyography analysis procedure
In order to measure muscle activity of the lower limbs during the walking on the underwater treadmill, we measured the activity for the medial gastrocnemius, rectus femoris, erector spinae, semitendinosus, tibialis anterior, vastus lateralis oblique. The EMG was measured using the waterproof Mini Wave (Cometa, Italy). Soft gaskets were used to make a water tight seal between the electrodes and the modules. All the electrodes were the Ag-AgCl electrode (Kendall H124SG, 30 × 24 mm). A specialized remote control was used to synchronize the signals between the modules and to start and stop the measurement. The data was stored in the memory device in each module and the data was transferred to the computer after completion of the measurements. All EMG data was sampled at 1,500 Hz and was filtered with 20~450 Hz bandpass, RMS as applied with a window size of 100 ms.
5. Statistical processing
SPSS (version 21.0 for windows) was used for all the statistical analysis including the calculation of the descriptive statistics providing the means and standard deviations for the 5 trials. One-way repeated measures ANOVA was used to calculate significant differences between the mean and standard deviation of the 3 conditions (over-ground walking, underwater walking, and underwater walking with an ankle weights). If a significant difference was established Post-test analysis was used to find the significant differences between the groups. A significance level of 0.05 was established to investigate if the differences were significant.
The results of the gait parameters are shown in the Tables 2 to 4.
|
Variable |
On-ground |
Underwater gait |
Underwater gait with |
F |
Post-hoc analysis |
|
|
Support phase (sec) |
Left side |
0.89±0.13 |
0.94±0.11 |
0.99±0.08 |
0.21 |
|
|
Right side |
0.87±0.05 |
1.05±0.27 |
1.05±0.27 |
2.11 |
||
|
Swing phase (sec) |
Left side |
0.41±0.03 |
0.68±0.08 |
0.70±0.08 |
53.19* |
a<b,a<c |
|
Right side |
0.37±0.04 |
0.65±0.10 |
0.69±0.06 |
65.99* |
a<b,a<c |
|
|
Step length (% height) |
Left side |
24.26±2.17 |
35.85±5.97 |
34.07±4.76 |
18.52* |
a<b,a<c |
|
Right side |
21.84±2.86 |
35.03±3.43 |
33.49±3.02 |
53.77* |
a<b,a<c |
|
|
Step rate (m/s) |
Left side |
1.18±0.13 |
0.93±0.11 |
0.93±0.09 |
16.59* |
a>b,a>c |
|
Right side |
1.33±0.12 |
0.99±0.13 |
0.95±0.08 |
35.61* |
a>b,a>c |
|
|
Variables |
On-ground |
Underwater |
Underwater gait with |
F |
Post-hoc |
|
|
Right support |
Knee |
146.21±76.83 |
64.58±57.66 |
201.89±46.15 |
12.59* |
a>b,b<c |
|
Ankle |
126.29±45.63 |
111.29±132.59 |
150.40±36.63 |
0.55 |
||
|
Hip |
100.58±48.98 |
65.42±55.50 |
115.75±21.34 |
3.37* |
a<c,b<c |
|
|
Right swing |
Knee |
290.57±54.49 |
195.01±22.29 |
80.52±55.21 |
50.93* |
a>b>c |
|
Ankle |
187.71±39.14 |
138.31±31.95 |
91.78±64.60 |
10.26* |
a>b,a>c |
|
|
Hip |
122.53±48.48 |
113.02±31.68 |
32.57±26.92 |
17.96* |
a>c,b>c |
|
|
Double stance |
Knee |
53.11±16.79 |
22.29±7.05 |
42.88±13.56 |
18.08* |
a>b,a>c |
|
Ankle |
36.63±11.58 |
61.47±19.44 |
41.27±13.05 |
0.66 |
||
|
Hip |
48.51±15.34 |
30.96±9.79 |
23.66±7.48 |
0.28 |
||
|
Variables |
On-ground |
Underwater |
Underwater gait with |
F |
Post-hoc |
|
Medial gastrocnemius |
100±0.00 |
115.80±28.75 |
135.26±36.19 |
3.506* |
a<c |
|
Rectus femoris |
100±0.00 |
145.53±37.77 |
185.04±65.90 |
7.532* |
a<b,a<c |
|
Erector spinae |
100±0.00 |
96.20±27.94 |
140.19±54.09 |
3.847 |
|
|
Semitendinosus |
100±0.00 |
117.44±44.17 |
162.75±50.02 |
5.655* |
a<c |
|
Tibialis anterior |
100±0.00 |
119.39±18.82 |
147.28±31.74 |
9.957* |
a<b,a<c |
|
Vastus lateralis oblique |
100±0.00 |
152.90±68.82 |
195.28±57.87 |
6.764* |
a<c |
|
Vastus medialis oblique |
100±0.00 |
147.01±39.56 |
184.06±52.03 |
9.971* |
a<b,a<c |
1. Gait parameters
The results of one-way ANOVA for walking time and distance showed statistically significant differences among the three conditions (p<0.05) for the step rate, step length and flight time. There were no statistically significant differences in contact time between the groups (F = 0.213, F = 2.114) for the support phase. The post-hoc revealed differences among the tested conditions for the support phase, step length and step rate.
2. Joint angular velocity for ankles, knee, and hip joints
The following results for the ankle, knee and hip joint angles are shown below for the right support phase, right swing phase and the double stance phase. For the right support phase there was significant differences between the three tested conditions for the knee and hip angular velocity (F = 12.597**, F = 3.370*). The results of the post-hoc analysis showed that the knee angular velocity was higher on the walking over ground (146.21 °/s ± 76.83 °/s) in comparison with the gait in water (64.58 °/s ± 2.179 °/s), but was largest while walking in water with the ankle weights (201.89 °/s ± 46.15 °/s). Similarly, the post hoc analysis showed that hip's angular velocity while walking in water with the ankle weights (115.75 °/s ± 21.34 °/s) was significantly higher than walking in water without the ankle weights (65.42°/s ± 55.50 °/s) and walking over-the-ground (100.58 °/s ± 48.98 °/s). For the right swing phase, there was significant differences between the three tested conditions for the knee, ankle and hip angular velocity (F = 50.932**, F = 10.265**, F = 17.969**).
The post-hoc analysis for the knee angular velocity showed the greatest increase in walking over-the-ground (290.57 °/s ± 54.49 °/s), followed by walking in water (195.01 °/s ± 22.29 °/s) and walking in water with the ankle weights (80.52 °/s ± 55.21 °/s). For the ankle angular velocity, the walking over-the-ground (187.71 °/s ± 39.14 °/s) increased more than the walking in water (138.31 °/s ± 31.95 °/s) and more than walking in water with the ankle weights (80.52 °/s ± 55.21 °/s). For the hip angular velocity, the post-hoc analysis showed that walking over-the-ground (122.53 °/s ± 48.48 °/s) was higher than both walking in the water with (113.02 °/s ± 31.68 °/s) and without the ankle weights (32.57 °/s ± 26.92 °/s). For the double stance phase the angular velocity of the knee was the only significant joint (F = 18.84**). The post-hoc analysis showed then knee angular velocity was highest from the over-the-ground (53.11 °/s ± 16.79 °/s), followed by the walking in the water with ankle weights (42.88 °/s ± 13.56 °/s), and then without ankle weights (22.29 °/s ± 7.05 °/s).
3. Maximum muscle activity for the lower limbs
The standardization of the EMG signal was performed using the % Reference Voluntary Contraction (RVC) method, which standardizes the reference voluntary contraction at 4 km/h of walking speed. The results of one-way ANOVA for the lower extremity muscles showed that the medial gastrocnemius, recuts femoris, semitendinosus, tibialis anterior, vastus lateralis oblique and vastus medialis oblique had statistically significant differences (F = 3.506*, F = 7.532**, F = 5.655*, F = 9.957**, F = 6.764**, F = 9.971**). As expected the muscle activity was found to be higher while walking in the water using the ankle weights. The results of the post-test are as follows. For the medial gastrocnemius, there was a significant increase of 35.26 ± 36.19% of muscle activity using the ankle weight during walking in water, but no significant difference increase in the walking in water. For the rectus femoris, there were significant increases for both the walking in water with and without the ankle weights (145.53 ± 37.77; 185.04 ± 65.90). For the erector spinae there was no significant differences recorded. For the Semitendinosus muscle there was a significance increase in the muscle activity for the walking with the ankle weight in water (162.75 ± 50.02%), and none for the walking in water. For the tibialis anterior there were significance increases shown for both with (147.28 ± 31.74) and without (119.39 ± 18.82) the ankle weights in water. For the vastus lateralis oblique there was a significant increase while using the ankle weight in water 195.28 ± 57.87%) but not without. Similarly, for the vastus medialis oblique there was a significant increase while using the ankle weight in water 184.06 ± 52.03%) but not without.
The purpose of this study was to investigate the change in gait kinematics and muscle activity (EMG) through the wearing effect of ankle weights, which is commonly used as supplementary exercise equipment, in underwater walking in healthy adult males. In this study, we focused from the perspective of improving one's gait pattern and walking in water as a type of rehabilitation exercise (Woo, Kang, & Kim, 2007), which shown improvements in gait speed and stride length. In addition, other researchers (Lee et al., 2009) showed similar positive effects of aquatic exercise as a form of rehabilitation training.
Among the kinematic variables, the swing time (time from toe off to heel contact) was significantly longer in the water because of water resistance, but the ankle weights have no significant influence on the swing time. In Nishiyori, Lai, Lee, Vrongistinos, & Jung (2016) study they reported the stride length and width, and walking speed were increased by in-water analysis using the ankle weights. However, in this in this study we used a different type of underwater treadmill, a manually moved treadmill, whereas Nishiyori et al. (2016) used a motorized treadmill. Both stride length and step rate decreased in the walking in water condition but the ankle weights did not significantly affect the length and speed. This means that our data portrays, that there is less movement per second while walking in the water as expected, which means that it uses more energy and is more effective for training the muscles.
During the right support phase, the angular velocity (maximum value) of the knee angular velocity was greater while using the ankle weights in water. The knee's angular velocity was even larger than walking on-the-ground. Likewise, for the hip joint's angular velocity there was an Increase walking with the ankle weights as opposed to walking on-the-ground. This can be explained that the ankle weights had more angular momentum and therefore the participant used more force to propel their legs forward. This phenomenon can be seen in a study of patients with hemiplegia, where Lee et al. (2009) reported that propulsion abilities were improved during toe off after partaking in an aquatic exercise gait program. This is due to the water regulating the speed of the heel contact during walking in the water, which reduces the momentum and thus requires more force to propel off the forefoot in the propulsion phase. These kinematic gait changes are however, not observed in the maximum angular velocity of the ankle joint between the three gait conditions. The lack of change in the ankle angular velocity may be use to the participants being healthy adult males with no disease affecting their ankle strength and coordination. During the right swing phase, the angular velocity of the knee, ankle, and hip were the highest whiles walking on the ground condition. This therefore, verifies that the resistance of the water as opposed to the air makes moving more difficult and slows down the participant so they can concentrate and focus on practicing their gait with more balance and coordinated movement, especially when they have the ankle weights in the water.
The activity of the lower extremity muscles (maximal value) was higher in the water with the ankle weights more than that of walking over-the-ground in the all six muscles except for the lumbar spine. The results of this study support Jung, Lee, Charalambous, & Vrongistinos (2010), who advocated that gait speed and strength increase after underwater treadmill gait training. In addition, a study of Nishiyori et al. (2016) in hemiplegic patients also found that aquatic exercise had the same positive effects on walking speed and strength. Clearly, aqua based gait training shows improvements in gait pattern characteristics but until now there have been no studies showing how gait in water affects the lower limb muscle activity which is vital for customizing effective rehabilitation programs for athletes and non-athletes alike.
In conclusion, the data from this study showed how walking in water with and without ankle weights can force changes in lower limb muscle activities, especially in medial gastrocnemius, recuts femoris, semitendinosus, tibialis anterior, vastus lateralis oblique and vastus medialis oblique. The ankle weight did not affect the muscle activity in the errector spinae which can be viewed positively as it shows that the ankle weights do not strain or overload the lower back. Knowing that ankle weights show an increase all the muscle activity compared to on-ground walking in the lower limbs it verifies that gait training in water is an effective way for the rehabilitation training of gait. The EMG does not show significant differences between aqua walking and the aqua walking with ankle weights, but the data shows a trend of increased EMG signal in all except the erector spinae. The gait kinematics between the conditions tested, show that the walking in the water increases the participant's stability and thus their stride length increases and the step rate reduces. Overall, this study shows that aqua-walking with ankle weights may be an effective way to help improve participant's gait patterns.
References
1. An, Y. D. (2003). Effects of the Aquatic Exercise and Weight Training for Physical Fitness of Patients with Middle Aged Man Lumbago. Journal of Sport and Leisure Studies, 19(2), 1301-1313.
Crossref
2. Chung, H. Y., Kim, S. K. & Chun, Y. J. (2011). The Effect of Water-based Exercise Program on Gait Coordination for People in Chronic Stroke. Journal of Sport and Leisure Studies, 43(2), 619-628.
Crossref
3. Danneskiold-Samsøe, B., Lyngberg, K., Risum, T. & Telling, M. (1987). The effect of water exercise therapy given to patients with rheumatoid arthritis. Scandinavian Journal of Rehabilitation Medicine, 19(1), 31-35.
Crossref
Google Scholar
4. Driver, S., O'Connor, J., Lox, C. & Rees, K. (2004). Evaluation of an aquatics programme on fitness parameters of individuals with a brain injury. Brain Injury, 18(9), 847-859.
Crossref
Google Scholar
5. Jung, T., Lee, D., Charalambous, C. & Vrongistinos, K. (2010). The influence of applying additional weight to the affected leg on gait patterns during aquatic treadmill walking in people poststroke. Archives of Physical Medicine and Rehabilitation, 91(1), 129-136.
Crossref
Google Scholar
6. Kim, E. H. (1998). Effect and Theory behind the Aqua-aerobics exercise. Rhumatism and Health Journal, 5(2), 296-302.
Crossref
7. Kim, K. E., Kim, H. M. & Woo, S. Y. (2006). The Effect of the Aqua-Rehabilitation Program on the Stroke Patient's Gait Patterns. The Korean Journal of Physical Education, 45(5), 449-455.
Crossref
8. Kim, H. J. & Choi, J. H. (2006). Effects of 12-week aquatic exercise on the isokinetic muscular function of knee joint in the elderly women. Korean Journal of Physical Education, 456(1), 655-664.
Crossref
9. Kim, S. K., Moon, J. H. & Yu, Y. J. (2014). Analysis of Gait Pattern on Hemiplegic Patients According to Condition of Water Height. Korean Journal of Sports Biomechanics, 16(3), 107-114.
Crossref
Google Scholar
10. Koury, J. M. (1996). Aquatic therapy programming: Guidelines for orthopedic rehabilitation. Human Kinetics Publishers.
Crossref
11. Lee, S. Y., Hyung, I. H. & Shim, J. M. (2009). The Effect of Aquatic Gait Training on Foot Kinesiology and Gait Speed in Right Hemiplegic Patients. Journal of Korean Contents, 9(12), 674 -682.
Crossref
Google Scholar
12. Nam, S. N., Kim, J. H. & Cho, Y. S. (2004). The Effect of Affected Side of Muscle Strength and Articular Moving Range of Persons with Cerebral Apoplexy Hemiplegia on Aqua-Rehabilitation. Korean Journal of Adapted Physical Activity, 12(2), 79-88.
Crossref
13. Nishiyori, R., Lai, B., Lee, D. K., Vrongistinos, K. & Jung, T. (2016). The use of cuff weights for aquatic gait training in people post-stroke with hemiparesis. Physiotherapy Research International, 21(1), 47-53.
Crossref
Google Scholar
14. Nielsen, C. R., Bates, C. A., Rooke, M. W., Hansen, F. R., Petersen, P. T., Le, M. V. & Lew, E. K. (1996). U.S. Patent No. 5,570,241. Washington, DC: U.S. Patent and Trademark Office.
Crossref
15. Park, S. W., Lee, K. J., Shin, D. C., Shin, S. H., Lee, M. M. & Song, C. H. (2014). The effect of underwater gait training on balance ability of stroke patients. Journal of Physical Therapy Science, 26(6), 899-903.
Crossref
Google Scholar
16. Ryu, J. C. & Kim, J. H. (2008). Kinematic analysis of gait pattern according to Load of %Wt of SCUBA subsidiaries' weights Loaded in underwater activities. Korean Journal of Physical Education, 47(1), 421-433.
Crossref
17. Svedenhag, J. & Seger, J. (1992). Running on land and in water: comparative exercise physiology. Medicine and Science in Sports and Exercise, 24(10), 1155-1160.
Crossref
Google Scholar
18. Wilder, D. G. (1993). The biomechanics of vibration and low back pain. American Journal of Industrial Medicine, 23(4), 577-588.
Crossref
Google Scholar
PubMed
19. Woo, S. Y., Kang, D. H. & Kim, H. J. H. (2007). A Gait Pattern Analysis of the Stroke Patients using the Aqua Rahabilitation program. SunchunYang University Science Journal, 13(2), 165-170.
Crossref
