Open Access, Peer-reviewed
eISSN 2093-9752
Open Access, Peer-reviewed
eISSN 2093-9752
Hye-In Lee
Bee-Oh Lim
http://dx.doi.org/10.5103/KJSB.2018.28.4.207 Epub 2019 January 17
Abstract
Objective: The purpose of this study was to examine the effects of an 8-week SMR, stretching, and band program on lower limb alignment (distance between the knees, Q angle) and gait (gait speed, stride length, impulse, and peak pressure) in female in their 20s who have genu varum.
Method: The participants, female in their 20s who had genu varum, were randomly divided into the SMR, Stretching, and Band group (SSB, n=9), Stretching and Band group (SB, n=9), and Control Group (CG, n=9). Experimental group A (SSB) performed 3 50-minute sessions of the program per week for 8 weeks while the experimental group B (SB) performed stretching and band correctional exercise in 3 40-minute sessions per week for 8 weeks. The control group had no correctional exercise program.
Results: Only the SSB group showed a significant increase in gait velocity and stride length in this study. The SSB and SB group showed a significant decrease of impulse on the forefoot after exercise program suggests that SMR and elastic band exercise had a positive effect on the distribution of foot pressure.
Conclusion: We concluded that 8-week genu varum correctional exercise program had beneficial effects on the gait parameters (gait velocity, stride length, impulse, peak pressure) in 20s women with genu varum.
Keywords
Self myofascial release Lower extremity alignment Gait Genu varum
Genu varum is a deformity marked by outward bowing at the knee, with both knees not touching each other while standing with legs closed (Park, Kong, Ko, Jang, & Park, 2015). Genu varum is particularly more prevalent among young women in their 20s than in men because of wearing high heels and crossing their legs to the side when sitting on the floor (Fraser et al., 2011). People with genu varum are easily fatigued, cannot walk for prolonged periods, and complain of numbing pain in both knee joints due to the ground reaction force vector was directed laterally (Saragaglia & Roberts, 2005). About 15-20% of the entire population present to the hospital with or make inquiries about genu varum (Woo, Lee, Lee, & Shim, 2016). Genu varum can be corrected either by non-surgical or surgical techniques. Non-surgical therapies include stretching, elastic band exercise, sling exercise, walking traction, muscle resistance exercise, chiropractic, chuna, and wearing corrective apparatus (Park et al., 2017). Stretching and elastic band exercise among the non-surgical treatments are interventions that are easy to be acces- sed (Park et al., 2017). The self myofascial release (SMR) technique corrects muscle imbalances, improves joint range of motion, relieves muscle soreness and joint stress, improves neuromuscular efficiency, relaxes muscles, provides optimal length-tension relationships (Cheatham & Kolber, 2017). Hence, this study presented SMR using foam rollers. Considering that genu varum is a knee dysarthrosis as well as a cause of abnormal gait, a concurrent investigation of lower limb alignment and ambulation is highly meaningful. The purpose of this study was to examine the effects of an 8-week SMR, stretching, and band program on lower limb alignment (distance between the knees, Q angle) and gait (gait speed, stride length, impulse, and peak pressure) in female in their 20s who have genu varum.
The participants, female in their 20s who had genu varum, were randomly divided into the SMR, stretching, and band group (SSB, n=9), stretching and band group (SB, n=9), and control group (CG, n=9). The inclusion criteria were as follows: female with genu varum (bow legs), defined as those with an inter-knee distance of greater than 5 cm when the medial malleolus of both legs are touching (Park et al., 2017); female without severe joint contracture in the lower limbs, visual disturbance, or peripheral vestibular disturbance; female who do not take drugs that influence balance; and female who provided informed consents to participate in the study. The genu varum correctional exercise program comprised SMR to increase muscular ROM, basic stretching of the adductor muscle, and exercise to strengthen the hip external rotator and lower limb muscles. Self myofascial release, elastic band and stretching exercise modified foam rolling-applying the technique of self-myofascial release, elastic band and stretching exercise based on NASM (national academy of sports medicine) (Yoo & Kim, 2015). The experimental group A (SSB) performed 3 50-minute sessions of the program per week for 8 weeks while the experimental group B (SB) performed stretching and band correctional exercise in 3 40-minute sessions per week for 8 weeks (Table 1). The control group had no correctional exercise program.
|
Type |
Frequency |
Time (min) |
|
|
Warm up |
- Dynamic stretching |
1 |
|
|
SMR (self-myofascial release) |
- Gastrocnemius/Soleus |
20 sec 1-times 2 sets |
8 |
|
- Adductors/Quadriceps |
|||
|
- Hamstring |
|||
|
- Tensor Fascia
Lata/lliotibal |
|||
|
- Piriformis/Gluteus |
|||
|
Stretching |
- Hamstring/Adductor |
15 sec 2-times 2 sets |
5 |
|
- Tensor Fascia Lata |
|||
|
- Piriformis |
|||
|
Elastic band |
- Hip external rotator |
15-times 2 sets |
35 |
|
- Gluteus maximus |
|||
|
- Quadriceps/Sartouris |
|||
|
- Rectus femoris |
|||
|
Cool down |
- Stretching |
1 |
Photographs were taken after placing stickers on the knees and pelvic bone to measure the distance between the knees. Q-angles were measured using kinematic analysis software, called Kinovea (Kinovea 0.8.15, free software). Kinovea is a video player for sport analysis. It provides a set of tools to capture, slow down, study, compare, annotate and measure technical performances. Kinovea system was verified of its reliability and validity (Sanchez et al., 2014). The angle between the line connecting centers of the anterior superior iliac spine and patella and the line connecting the tibial tuberosity to the center of the patella was measured using Kinovea software (Sanchez et al., 2014). The GAITRite system (CIR Systems Inc. Peekskill, NY), which was verified of its reliability and validity as a tool to objectively assess spatio-temporal variables of gait and pressure distributions (impulse) of the feet, was used to measure gait parameters (McDonough et al., 2001). Two-way repeated measures ANOVA was performed with group (SSB, SB, and CG) and exercise program for genu varum (pre- and post-) as the independent variables. Statistical analyses were performed using SPSS 21.0 software. Trends and tendencies were analyzed using the interaction graph when ANOVA results showed an interaction effect between the two independent variables, and only the main effect was verified when no interaction effect existed. The Tukey's test was performed as a post-hoc test, and statistical significance was set to α=.05.
1. Lower limb alignment variables (Inter-knee distance, Q-angle)
Repeated measures ANOVA showed that there was no time and group interaction effect (p>.05) in inter-knee distance and q-angle. Further, main effects of time and group were not statistically significant in all three groups in inter-knee distance and q-angle (p>.05) (Table 2).
|
Inter-knee distance |
q-angle |
|||
|
Pre |
Post |
Pre |
Post |
|
|
SSB |
5.307±0.89 |
4.531±0.59 |
19.43±0.98 |
18.14±1.21 |
|
SB |
5.047±0.76 |
4.779±0.53 |
18.67±1.03 |
18.33±0.82 |
|
CG |
5.333±0.97 |
5.655±0.82 |
19.13±1.13 |
19.67±0.58 |
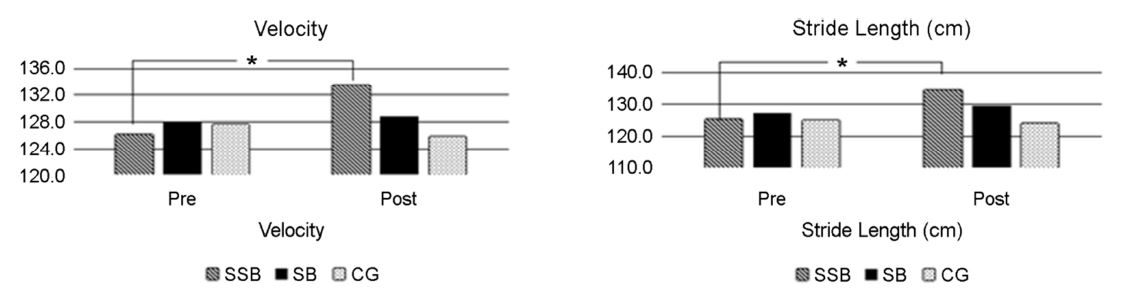
2. Gait variables (Gait velocity, Stride length)
Repeated measures ANOVA showed that there was no significant time and group interaction effect (p>.05). The main effect of time was significant in the SSB group, where gait velocity and stride length significantly increased after exercise compared to that before exercise (p<.05; Figure 1). Post-hoc test for group effect showed that there were no significant differences among the three groups (p>.05).
3. Impulse (P*T)
Repeated measures ANOVA showed that there was a significant time and group interaction effect in the forefoot (front area of foot) section (p<.05). Although there were no significant differences among the three groups before training, the impulse in the forefoot section significantly decreased after training in the SSB and SB groups. As shown in Table 3, there was a time and group interaction effect in the hindfoot (rear area of foot) section (p<.05). Although there were no significant differences among the three groups before training, the impulse in the hindfoot section significantly increased after training in the SSB groups. There was a time and group interaction effect in the medialfoot (medial area of foot) and lateralfoot (lateral area of foot) section (p<.05). And there were no significant differences among the three groups before and after training in the medialfoot and lateralfoot section (p<.05).
|
Impulse (P*T) |
Ratio of Hind/Forefoot |
Peak pressure |
||||
|
Forefoot |
Pre |
Post |
Pre |
Post |
Pre |
Post |
|
SSB |
51.87±5.05 |
45.12±3.95* |
48.41 |
63.43 |
47.47±2.97 |
45.71±5.72 |
|
SB |
51.06±3.58 |
47.36±3.21* |
50.53 |
57.79 |
48.88±3.27 |
45.70±2.65* |
|
CG |
50.59±3.96 |
50.76±8.15 |
52.03 |
51.36 |
47.79±1.58 |
46.48±6.12 |
|
Hindfoot |
Pre |
Post |
|
Pre |
Post |
|
|
SSB |
25.11±3.93 |
28.62±2.95* |
|
23.24±3.05 |
27.51±7.02 |
|
|
SB |
25.80±2.44 |
27.37±1.99 |
|
23.12±3.09 |
26.32±4.05 |
|
|
CG |
26.32±2.60 |
26.07±5.09 |
|
23.66±2.51 |
22.83±6.26 |
|
|
Medialfoot |
Pre |
Post |
|
Pre |
Post |
|
|
SSB |
45.76±2.38 |
47.23±4.23 |
|
47.12±3.48 |
49.50±1.92 |
|
|
SB |
45.86±2.24 |
45.90±5.56 |
|
47.08±2.73 |
47.60±4.15 |
|
|
CG |
46.62±3.11 |
46.47±5.60 |
|
47.79±2.47 |
47.57±2.76 |
|
|
Lateralfoot |
Pre |
Post |
|
Pre |
Post |
|
|
SSB |
54.36±2.37 |
54.37±3.08 |
|
52.98±3.45 |
51.31±2.01 |
|
|
SB |
54.86±2.12 |
54.14±5.51 |
|
53.01±2.78 |
52.54±4.17 |
|
|
CG |
54.61±2.67 |
54.61±2.67 |
|
53.19±2.45 |
52.60±2.70 |
|
4. Peak pressure
Repeated measures ANOVA showed that there were no significant time and group interaction effects in the forefeet section (p>.05). Dependent t-test for time showed that the peak pressure significantly decreased after training in the SB group (p<.05). Although there were no significant differences among the three groups before training, the peak pressure in the hindfoot section increased after training in the SSB and SB groups (Table 3).
Although inter-knee distances were not significantly different among the three groups, it decreased from 5.307 to 4.531 cm in the SSB group (0.776 cm) and from 5.047 to 4.779 cm in the SB group (0.268 cm), suggesting that the amount of reduction was larger in the SSB group. Our exercise program was designed to relax the hamstring while strengthening the quadriceps to improve the inter-knee distance. Shortening of the hamstring decreases knee ROM, increasing the load on the knee joint and leading to genu varum (Greene, 1996). Normalizing knee ROM is essential for correction of genu varum (Cheatham et al., 2015; MacDonald et al., 2013), and SMR using foam rollers increases ROM and enhances flexibility (Beardsley & Skarabot, 2015; Cheatham et al., 2015). MacDonald et al. (2013) reported that 1-minute SMR on the hamstring of 11 healthy male subjects led to an 8~10 degree increase of ROM, and SMR on the hamstring using foam rollers also led to a greater reduction of knee distance in the SSB group than in the SB group in our study. This finding suggests that SMR is more effective than stretching in enhancing flexibility (Skarabot, Beardsley, & Stirn, 2015). Weakening of the quadriceps brings about changes in the body's alignment axis, potentially causing problems in the lower limb alignment (Beardsley & Skarabot, 2015). Ballal et al. (2010) mentioned that quadriceps should be strengthened with elastic band exercises to stabilize the knee joint. In our study, strengthening the quadriceps using elastic bands led to reduction of inter-knee distance in the SSB and SB groups.
Although statistically insignificant, Q-angles decreased from 19.43 to 18.14° in the SSB group (1.29°) and from 18.67 to 18.33° in the SB group (0.43°), becoming closer to the normal angle of 16° with a greater reduction in the SSB group. Our exercise program was designed to relax the iliotibial band while strengthening the hip external rotator to improve the Q-angle, based on a previous report that the Q-angle can be corrected by strengthening the hip external rotator and stretching the iliotibial band (Heath & Staheli, 1993). Applying fascial massage on runners with iliotibial band syndrome alleviated their knee pain (Cheatham et al., 2015), and the same study suggested the use of foam rollers in follow-up studies. From this perspective, our study is meaningful in that we used foam rollers to relax the iliotibial band. Further, we used elastic bands to strengthen weakened hip external rotator. Repetitive resistance training involving weakened external rotator muscle has been reported to have remarkable effects in correcting genu varum, and strengthening of the external rotator muscle using elastic bands was reported to decrease the Q-angle in patients with genu varum (Lee et al., 2015), which were in line with the findings of the present study. However, considering the Q-angle remains markedly above the normal angle, a more effective exercise program should be developed with a long-term design as opposed to a short-term application.
Only the SSB group showed a significant increase in gait velocity and stride length in this study. The exercise program used in this study was designed to relax the tensor of fascia lata and strengthen hip muscles to improve stride length and gait velocity. Shortened tensor of fascia lata induces internal rotation of the hip joint, and particularly, it can exacerbate the abnormal alignment during repetitive movement, such as walking (Schroeder & Best, 2015). The fact that only the SSB group showed significant differences suggest that SMR using foam rollers is more effective in enhancing flexibility (Schroeder & Best, 2015). Strengthening lower limb muscles improved gait performance, as was previously suggested that elastic band exercise had positive effects on gait performance (Ballal et al., 2010). In our study, strengthening of hip muscles increased gait velocity and stride length, and improvement of gait velocity is related to strengthening of lower limb muscles (Van Gheluwe et al., 2005). There were no exercise effect on the changes in inter-knee distance and Q angle. However, there were significant increases in gait velocity and stride length in the group of SSB. In addition, this SSB group showed decreased forefoot impulse but increased hindfoot impulse. Generally, there is a positive relationship between gait velocity and impulse. This controversial result showed due to increased walking velocity after exercise program.
The time and group interaction effect on the impulse was significant in the forefoot and hindfoot sections, but not on the medial and lateral sections. A 6:4 pressure distribution to the forefoot and hindfoot is the ideal feet pressure distribution (Webster et al., 2005). In the participants of our study, feet pressure was concentrated in the forefoot, and due to the typical posture of genu varum, center of mass was focused on the front of the feet due to an excessive extension of the knee. Muscles that are related to the impulse in this study are the gastrocnemius and soleus. Shortening of the soleus muscle induces pes cavus and increases the shock felt against the ground during ambulation, increasing fatigue. Relaxation of the soleus muscle produced by our exercise program led to a reduction of pressure on the forefoot to near-normal levels, from 48.41% to 63.43% in the SSB group and from 50.53% to 57.79% in the SB group. Furthermore, the fact that only the SSB group showed a significant increase of pressure on the hindfoot suggest that SMR had a positive effect on the distribution of foot pressure. Elastic band exercise in women with genu varum produced beneficial effects on balance of foot pressure significantly reducing pressure on the forefoot while significantly increasing pressure on the hind- foot by stretching the soleus muscle (Ballal et al., 2010). Although there were no significant differences among the three groups before training, pressure on the medial section increased by 1.47 N · s and 0.07 N · s in the SSB and SB group, respectively, and the pressure in the lateral section reduced by 0.10 N · s and 0.72 N · s in the SSB and SB groups, respectively. Medial pressure increases while lateral pressure decreases with increasing gait velocity (Youdas et al., 2006). The exercise program to correct genu varum increased the participants' gait velocity, thereby normalizing their feet pressure distribution.
This study aimed at examining the effects of an 8-week exercise program to correct genu varum on lower limb alignment (inter-knee distance, Q-angle) and gait (gait velocity, stride length, impulse, peak pressure) in women in their 20s with genu varum, and the following conclusions were drawn. The SSB group showed significantly higher gait velocity and stride length after training. The impulse on the forefoot section significantly decreased after training in the SSB and SB groups. The impulse on the hindfoot significantly increased after training in the SSB group. Peak pressure in the forefoot section significantly decreased after an 8-week genu varum correction program in the SB group. In conclusion, an 8-week genu varum correction exercise program had beneficial effects on the gait parameters (gait velocity, stride length, impulse, peak pressure) in 20s women with genu varum. In future studies, foam rollers should be compared with other tools for SMR on a large enough sample to validate the effectiveness of exercise pro- grams to correct genu varum as well as to identify more effective SMR techniques.
References
1. Ballal, M. S., Bruce, C. E. & Nayagam, S. (2010). Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates. Journal of Bone and Joint Surgery, 92(2), 273-276.
Crossref
Google Scholar
2. Beardsley, C. & Skarabot, J. (2015). Effects of self-myofascial release: A systematic review. Journal of Bodywork and Movement Therapies, 19(4), 747-758.
Crossref
Google Scholar
PubMed
3. Cheatham, S. W. & Kolber, M. J. (2017). Does Self-Myofascial Release With a Foam Roll Change Pressure Pain Threshold of the Ipsilateral Lower Extremity Antagonist and Contralateral Muscle Groups? An Exploratory Study. Journal of Sport Rehabilitation, 1-18.
Crossref
4. Cheatham, S. W., Kolber, M. J., Cain, M. & Lee, M. (2015). The Effects of Self-Myofascial Release Using a Foam Roll or Roller Massager on Joint Range of Motion, Muscle Recovery, and Performance: A Systematic Review. International Journal of Sports Physical Therapy, 10(6), 827-838.
Crossref
Google Scholar
5. Fraser, S. C., Neubauer, P. R. & Ain, M. C. (2011). The role of arthrography in selecting an osteotomy for the correction of genu varum in pediatric patients with achondroplasia. Journal of Pediatric Orthopaedics, 20(1), 14-16.
Crossref
Google Scholar
6. Greene, W. B. (1996). Genu varum and genu valgum in children: differential diagnosis and guidelines for evaluation. Comprehensive Therapy, 22(1), 22-29.
Crossref
Google Scholar
7. Heath, C. H. & Staheli, L. T. (1993). Normal limits of knee angle in white children--genu varum and genu valgum. Journal of Pediatric Orthopaedics, 13(2), 259-262.
Crossref
Google Scholar
PubMed
8. McDonough, A. L., Batavia, M., Chen, F. C., Kwon, S. & Ziai, J. (2001). The validity and reliability of the GAITRite system's measurements: A preliminary evaluation. Archives of Physical Medicine and Rehabilitation, 82(3), 419-425.
Crossref
Google Scholar
9. MacDonald, G. Z., Penney, M. D., Mullaley, M. E., Cuconato, A. L., Drake, C. D., Behm, D. G. & Button, D. C. (2013). An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. Journal of Strength and Conditioning Research, 27(3), 812-821.
Crossref
Google Scholar
10. Park, S., Kong, Y. S., Ko, Y. M., Jang, G. U., & Park, J. W. (2015). Differences in onset timing between the vastus medialis and lateralis during concentric knee contraction in individuals with genu varum or valgum. Journal of Physical Therapy Science, 27(4), 1207-1210.
Crossref
Google Scholar
11. Park, S. R., Ro, H. L. & Nankoong, S. (2017). The Effect of Stretching and Elastic Band Exercises Knee Space Distance and Plantar Pressure Distribution during Walking in Young Individuals with Genu Varum. Journal of the Korean Society of Physical Medicine, 12(1), 83-91.
Crossref
Google Scholar
12. Sanchez, H. M., Sanchez, E. G., Baraúna, M. A. & Canto, R. S. (2014). Evaluation of Q angle in differents static postures. Acta Ortopedica Brasileira, 22(6), 325-329.
Crossref
Google Scholar
13. Saragaglia, D. & Roberts, J. (2005). Navigated osteotomies around the knee in 170 patients with osteoarthritis secondary to genu varum. Orthopedics, 28(10 Suppl), s1269-1274.
Crossref
Google Scholar
14. Schroeder, A. N. & Best, T. M. (2015). Is self myofascial release an effective preexercise and recovery strategy? A literature review. Current Sports Medicine Reports, 14(3), 200-208.
Crossref
Google Scholar
15. Skarabot, J., Beardsley, C. & Stirn, I. (2015). Comparing the effects of self-myofascial release with static stretching on ankle range-of-motion in adolescent athletes. International Journal of Sports Physical Therapy, 10(2), 203-212.
Crossref
Google Scholar
16. Van Gheluwe, B., Kirby, K. A. & Hagman, F. (2005). Effects of simulated genu valgum and genu varum on ground reaction forces and subtalar joint function during gait. Journal of the American Podiatric Medical Association, 95(6), 531-541.
Crossref
Google Scholar
17. Webster, K. E., Wittwer, J. E. & Feller, J. A. (2005). Validity of the GAITRite walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture, 22(4), 317-321.
Crossref
Google Scholar
PubMed
18. Woo, K., Lee, Y. S., Lee, W. Y. & Shim, J. S. (2016). The Efficacy of Percutaneous Lateral Hemiepiphysiodesis on Angular Correction in Idiopathic Adolescent Genu Varum. Clinics in Orthopedic Surgery, 8(1), 92-98.
Crossref
Google Scholar
19. Yoo, B. G. & Kim, E. H. (2015). The effects of the correction exercise program combined with stretching and elastic band exercise on femoral intercondylar distance, Q-angle, plantar pressure in under- graduate with genu varum. Journal of the Korea Academia-Industrial cooperation Society, 16(3), 2064-2072.
Crossref
Google Scholar
20. Youdas, J. W., Hollman, J. H., Aalbers, M. J., Ahrenholz, H. N., Aten, R. A. & Cremers, J. J. (2006). Agreement between the GAITRite walkway system and a stopwatch-footfall count method for measurement of temporal and spatial gait parameters. Archives of Physical Medicine and Rehabilitation, 87(12), 1648-1652.
Crossref
Google Scholar
